In this story about small town stranger appreciation, a mom learns lessons while her little kid grows up a little more, making kind decisions about safety, cats, and personal capabilities. Let’s nurture our relationships and read on. To begin, why is this balloon in the bathtub?
Short answer: to protect our cat (Rolo, who can open every door except a shower door) from GI distress caused by eating the string.
Long answer: My 4-year old son is building resilience, self-discipline, confidence, and communication skills. Today, he acquired a balloon from a Habitat for Humanity kiosk at the local Berthoud farmer’s market (which makes up for its well-known lack of vegetables by being located at the new splash pad park, bringing multiple sourdough purveyors, and hosting the beloved Wildfire Arts kids art table. Today there were even dancing local ladies and a massive drum circle. And it’s really not the town’s fault about the veggies. We have a notoriously short growing season, etc etc).
My kids love balloons. Yes, I know they’re dangerous… a family I know had a child fall from a large mylar one at his own party and get seriously injured. In our family we aren’t allowed to put them up to our mouths, and so on. Mine play with them a few times a year under supervision…. STRONG supervision. This is partly because we have a large cat who loves to eat that curly, delicious, devilish shreddable balloon string. He gets very sick from eating it, and he just can’t stop. If it’s in the house, he’s gonna find it and have it for his own.
So we got a balloon anyway. They were gleeful, knowing this was rare. The kids ran to the playground, clutching their strings. Enter some sort of spinning playground equipment and a spill. No scrapes, no blood, no bump… but snap! My son’s balloon was gone like that, soaring to the sky as if we’d meant to poison nature. I’m so sorry, birds. I really should have known.
Well, there was another family observing. I’m not going to say they caused the disaster, but they sure fixed it. (In truth, a park dad had been giving all the kids massive pushes on this spinning piece of park equipment, which led to riotous laughter and a moment for me to call my own father to check on him after some difficult health issues early this month). I saw the spill, the cut string, the loss all play out in slow motion and was ready when my 4 year old sprinted to me screaming as I slammed my finger down on the phone fast to spare my dad the screams in his phone ear. Are you hurt? “No.” Are you ok? “NO!”
That darn balloon. I went into triage mode. The kids were given some options from which to pick (stay here and play a little but we have to use nature friendly voices again; taste a pickle and calm down with mom; go home right away, etc). Kid opted for a pickle and kid 2 went on spinning, her balloon much more securely attached to her hat band. It’s a pink cowgirl hat and she is NOT taking that thing off. But her 4-year old brother was SO SAD.
You know those moments, parents? You know when you COULD go get another (whatever spilled-melted-dropped-broken-ruined) thing, but it’s a long way away, and isn’t there a lesson here crammed in there that you don’t want to miss and don’t want your kid to miss? (And what about the voice from your past reminding you that when you were a kid and that lady next to you at Disney broke your balloon with her 1980’s cigarette and she didn’t apologize and your parents did not buy you a new one and how will he learn a lesson if you don’t inflict on him the pain you felt when you were 6… just me? To be fair, I didn’t remember it. My dad reminded me about it later as I recounted the blue balloon story.)
“OK but mom, it was not his fault!” my brain argued. “He fell and the string broke and he. is. SO. SAD!”
Yet I stuck to my proverbial guns. I wasn’t mean, I was soft and sympathetic, walking with my crying kid back to the car as he suffered loudly and his sister bounced along with her balloon. And guess what happened before we left the parking lot? If you live in Berthoud maybe you already guessed.
The stranger family re-appeared. One of the kids was clutching a lollipop- Oh please don’t let my kids notice that, I prayed. Too late, my daughter instantly said the quiet part out loud. But that didn’t matter, because… the stranger-family-dad (sorry kind sir, this is what my children have dubbed you) was holding out a balloon. “He took a pretty big spill back there,” he said apologetically. “We decided we didn’t want him to have to leave without a balloon.”
Glory be! Is this the small town feeling creeping up my arms, a mix of chill bumps and gratefulness and humanity and embarrassment (my toddler was just about to leave without one and darn it I was going to make sure he was ok with that)?
We humbly and gratefully said big thank yous. My little guy’s eyes were dazzling blue worlds of gratitude staring up at this family, accepting his balloon. He clutched the string like I clutch his hand at Trail Ridge Road overlooks while we stare over the edge.
There were so many lessons today. First, the amazement of my son: “I didn’t realize a stranger would be so kind to another stranger!” Then, the detailed discussion of situations when it is ok, versus not ok, to take things from strangers. We discussed the role of my presence, of the dad asking me “can I give this to him?”, and other nuanced questions only a 4- and 6-year-old can generate. We rode home happy.
And now it was nap time. Here’s where his character development really comes into the story. “Mom,” he said sleepily, “I really, really love playing with the balloon. So I think we better work together to find a safe place that is not inside my room. Especially for Rolo. Can you help?”
Yes, son. I got your back on this one. He’s asleep now, napping after all the excitement, while the cat lies in wait outside the bathtub and I take in the wonder that is 4-year-olds growing up.
Oh… and I love other families as well. I provide mentoring to families, therapists and teams that gives them the tools to transcend trauma. See my courses at www.cuspemergenceuniversity.com, join a group with me, book an appointment, or just email me any time.
Article in series on TIBA (trauma-informed behavior analysis) by Dr. Teresa Camille Kolu, Ph.D., BCBA-D
For many people including up to 90% of autistic women, our behaviors, moods, and medical symptoms worsen every month in the luteal phase of the menstrual cycle. But why? This may baffle even the most highly trained OBGYNs and behavioral scientists, let alone parents, caregivers, staff, and clients receiving behavioral services.
To Dr. Kolu, behavioral seismology is the scientific study of cyclical changes in a person’s experience that result in predictable (and potentially damaging) disruptions in an individual’s behavioral environment. Predictions about cyclical needs could be used to reduce the risk of damage and injury to clients and others related to hormone-behavior interactions. People can experience an increase in behavior needs, emotional needs, medical needs, and challenging interactions between all three, but it can help to know and be able to predict when they will be most at risk.
For individuals assigned female at birth (and relevant to anyone who loves, cares for, or conducts behavioral support for someone with these characteristics) , Dr. Camille Kolu discusses these four distinct behavioral risk profiles as ways to help make sense of the predictable disruptions that can occur regularly and monthly for up to 2 weeks at a time (as in PMDD) or for several years (as in perimenopause). The 4 risk profiles include the following:
PCOS or polycystic ovary syndrome
PMDD or premenstrual dysphoric disorder
Perimenopause and
PME (premenstrual exacerbation).
These 4 profiles are each accompanied by a pdf fact sheet downloadable as a resource in the new course on Behavioral Seismology from Cusp Emergence University. In each PDF are characteristic risk factors; biological signs; medical, behavioral and other symptoms the risk profile makes more likely; a to-do list for providers; and notes on expected interactions between behavior and the medical diagnosis. For instance, in PCOS, a client in behavioral services might experience self-injury related to the predictable pain during ovulation or food related behavior challenges that are related to the characteristic insulin resistance. In PMDD, a client in behavioral services who also has autism might experience sudden explosive outbursts in the second half of their menstrual cycle.
What are some of the benefits of becoming a healthcare or behavioral provider more informed about behavioral seismology?
Information can help to demystify behavior needs, as we put them into the context of an individual suffering with medical issues that need treatment. As a case example, one of Dr. Kolu’s patients had a diagnosis of PCOS (polycystic ovary syndrome) and took related medication. However, the behavioral team thought of that diagnosis as completely divorced from their behavioral treatment, and had never been trained on (or requested support to learn) what specific behaviors were anticipated and when they would get worse. As a result, the behavioral team had written goals that were inappropriate and inflexible. In most of the risk profiles we discuss in the Behavioral Seismology course, behaviors improve for the first two weeks of the cycle, when reinforcers are more potent. In the luteal phase of the cycle, a behavior targeted for reduction is likely to come raging back, as several things occur: one of the most significant is that aversive stimuli are temporarily more aversive! Another is that conditioning processes (such as extinction) are affected by hormone levels; for someone with trauma, the things we call “conditioned fear stimuli” or reminders of bad things that happened in the past, seem more present and potent during the luteal phase. Could these changes affect behavior? Absolutely! What if we ignored these biological realities and expected clients to simply do better and better on their goals in a linear trajectory? Could this be demoralizing for them and frustrating for caregivers and uninformed providers?
We can be more flexible in goal writing, more appropriate in support, more predictive in funding needs, and more compassionate in treatment, when we truly take someone’s medical needs into account. This is the point of the Behavior Analysis Certification Board (BACB)’s Ethics Code Item 2.12. For providers interested in taking that code seriously, Behavioral Seismology (4 CEUs total) provides an ethics CEU focused on treating behavior in ways much more contextually appropriate.
Other things you’ll find in the course:
4 pdf risk profiles
An aversive stimulus tracker template (and filled out example)
A Cyclical Needs Conversation Guide for providers
A tool called “Rethink Your Language” (using the example of how the word “aggression” can cause impactful changes in someone’s life)
Insulin Resistance Handout (with information about how this condition intersects with each risk profile discussed in the training)
Information on how autism intersects in surprising ways with several of the risk profiles (and a tool called “Acting on Combined Risk”)
A Cyclic Behavior Support Plan Template
The Cyclic Systems Support Checklist (for companies and teams making these changes in their processes)
A video script for the 8 videos accompanied by printable handouts
Full references for over 70 published articles (including ones by autistic providers on lived experiences of individuals affected by both autism and hormone-behavior interactions
Thought questions
Thoughtful intersections and objectives to apply ethics codes to understanding the ethical implications of information in each chapter
and much more.
Want to learn more? Take the course, contact Dr. Kolu to let us know you want to attend one of our live training sessions on Behavioral Seismology, or see the references below.
Beltz, A. M., Corley, R. P., Wadsworth, S. J., DiLalla, L. F., & Berenbaum, S. A. (2020). Does puberty affect the development of behavior problems as a mediator, moderator, or unique predictor?. Development and psychopathology, 32(4), 1473-1485.
Graber JA (2013). Pubertal timing and the development of psychopathology in adolescence and beyond. Hormones and Behavior, 64(2), 262–269.
Negriff S, & Susman EJ (2011). Pubertal timing, depression, and externalizing problems: A framework, review, and examination of gender differences. Journal of Research on Adolescence, 21(3), 717–746. doi: 10.1111/j.1532-7795.2010.00708.x
References for PCOS:
Cherskov, A., Pohl, A., Allison, C., Zhang, H., Payne, R. A., & Baron-Cohen, S. (2018). Polycystic ovary syndrome and autism: a test of the prenatal sex steroid theory. Translational psychiatry, 8(1), 136.
Dan, R., Canetti, L., Keadan, T., Segman, R., Weinstock, M., Bonne, O., … & Goelman, G. (2019). Sex differences during emotion processing are dependent on the menstrual cycle phase. Psychoneuroendocrinology, 100, 85-95.
Dumesic, D. A., & Lobo, R. A. (2013). Cancer risk and PCOS. Steroids, 78(8), 782-785.
Evans, S. M., & Foltin, R. W. (2006). Exogenous progesterone attenuates the subjective effects of smoked cocaine in women, but not in men. Neuropsychopharmacology, 31(3), 659-674.
Evans, S. M., Haney, M., & Foltin, R. W. (2002). The effects of smoked cocaine during the follicular and luteal phases of the menstrual cycle in women. Psychopharmacology, 159, 397-406.
Katsigianni, M., Karageorgiou, V., Lambrinoudaki, I., & Siristatidis, C. (2019). Maternal polycystic ovarian syndrome in autism spectrum disorder: a systematic review and meta-analysis. Molecular psychiatry, 24(12), 1787-1797.
Mulligan, E. M., Nelson, B. D., Infantolino, Z. P., Luking, K. R., Sharma, R., & Hajcak, G. (2018). Effects of menstrual cycle phase on electrocortical response to reward and depressive symptoms in women. Psychophysiology, 55(12), e13268.
Sakaki, M., & Mather, M. (2012). How reward and emotional stimuli induce different reactions across the menstrual cycle. Social and personality psychology compass, 6(1), 1-17.
References for PMDD:
Browne, T. K. (2015). Is premenstrual dysphoric disorder really a disorder? Journal of Bioethical Inquiry, 12, 313-330.
Ellis, R., Williams, G., Caemawr, S., Craine, M., Holloway, W., Williams, K., … & Grant, A. (2025). Menstruation and Autism: a qualitative systematic review. Autism in Adulthood.
Epperson, C. N., Pittman, B., Czarkowski, K. A., Stiklus, S., Krystal, J. H., & Grillon, C. (2007). Luteal-phase accentuation of acoustic startle response in women with premenstrual dysphoric disorder. Neuropsychopharmacology, 32(10), 2190-2198.Ford, 2012
Freeman, E. W., & Sondheimer, S. J. (2003). Premenstrual dysphoric disorder: recognition and treatment. Primary care companion to the Journal of clinical psychiatry, 5(1), 30.
Gingnell, M., Bannbers, E., Wikström, J., Fredrikson, M., & Sundström-Poromaa, I. (2013). Premenstrual dysphoric disorder and prefrontal reactivity during anticipation of emotional stimuli. European Neuropsychopharmacology, 23(11), 1474-1483.
Halbreich, U., Borenstein, J., Pearlstein, T., & Kahn, L. S. (2003). The prevalence, impairment, impact, and burden of premenstrual dysphoric disorder (PMS/PMDD). Psychoneuroendocrinology, 28, 1-23.
Kulkarni, J., Leyden, O., Gavrilidis, E., Thew, C., & Thomas, E. H. (2022). The prevalence of early life trauma in premenstrual dysphoric disorder (PMDD). Psychiatry research, 308, 114381.
Obaydi, H., & Puri, B. K. (2008). Prevalence of premenstrual syndrome in autism: a prospective observer-rated study. Journal of International Medical Research, 36(2), 268-272.
Protopopescu, X., Tuescher, O., Pan, H., Epstein, J., Root, J., Chang, L., … & Silbersweig, D. (2008). Toward a functional neuroanatomy of premenstrual dysphoric disorder. Journal of affective disorders, 108(1-2), 87-94.
Sacher, J., Zsido, R. G., Barth, C., Zientek, F., Rullmann, M., Luthardt, J., … & Sabri, O. (2023). Increase in serotonin transporter binding in patients with premenstrual dysphoric disorder across the menstrual cycle: a case-control longitudinal neuroreceptor ligand positron emission tomography imaging study. Biological Psychiatry, 93(12), 1081-1088.
References for Perimenopause:
Ambikairajah, A., Walsh, E., & Cherbuin, N. (2022). A review of menopause nomenclature. Reproductive health, 19(1), 29.
Arnot, M., Emmott, E. H., & Mace, R. (2021). The relationship between social support, stressful events, and menopause symptoms. PloS one, 16(1), e0245444.
Avis, N. E., Crawford, S. L., Greendale, G., Bromberger, J. T., Everson-Rose, S. A., Gold, E. B., … & Study of Women’s Health Across the Nation. (2015). Duration of menopausal vasomotor symptoms over the menopause transition. JAMA internal medicine, 175(4), 531-539.
Constantine, G. D., Graham, S., Clerinx, C., Bernick, B. A., Krassan, M., Mirkin, S., & Currie, H. (2016). Behaviours and attitudes influencing treatment decisions for menopausal symptoms in five European countries. Post Reproductive Health, 22(3), 112-122.
Cusano, J. L., Erwin, V., Miller, D., & Rothman, E. F. (2024). The transition to menopause for autistic individuals in the US: a qualitative study of health care challenges and support needs. Menopause, 10-1097.
Duralde, E. R., Sobel, T. H., & Manson, J. E. (2023). Management of perimenopausal and menopausal symptoms. Bmj, 382.
Guthrie, J. R., Dennerstein, L., Taffe, J. R., & Donnelly, V. (2003). Health care-seeking for menopausal problems. Climacteric, 6(2), 112-117.
Hamilton, A., Marshal, M. P., & Murray, P. J. (2011). Autism spectrum disorders and menstruation. Journal of adolescent health, 49(4), 443-445.
Hoyt, L. T., & Falconi, A. M. (2015). Puberty and perimenopause: reproductive transitions and their implications for women’s health. Social science & medicine, 132, 103-112.
Karavidas, M., & de Visser, R. O. (2022). “It’s not just in my head, and it’s not just irrelevant”: autistic negotiations of menopausal transitions. Journal of Autism and Developmental Disorders, 52(3), 1143-1155.
Kling, J. M., MacLaughlin, K. L., Schnatz, P. F., Crandall, C. J., Skinner, L. J., Stuenkel, C. A., … & Faubion, S. S. (2019, February). Menopause management knowledge in postgraduate family medicine, internal medicine, and obstetrics and gynecology residents: a cross-sectional survey. In Mayo Clinic Proceedings (Vol. 94, No. 2, pp. 242-253). Elsevier.
Moseley, R. L., Druce, T., & Turner-Cobb, J. M. (2020). ‘When my autism broke’: A qualitative study spotlighting autistic voices on menopause. Autism, 24(6), 1423-1437.
Moseley, R. L., Druce, T., & Turner‐Cobb, J. M. (2021). Autism research is ‘all about the blokes and the kids’: Autistic women breaking the silence on menopause. British Journal of Health Psychology, 26(3), 709-726.
Namazi, M., Sadeghi, R., & Behboodi Moghadam, Z. (2019). Social determinants of health in menopause: an integrative review. International journal of women’s health, 637-647.
Ohayon, M. M. (2006). Severe hot flashes are associated with chronic insomnia. Archives of internal medicine, 166(12), 1262-1268.
O’Reilly, K., McDermid, F., McInnes, S., & Peters, K. (2023). An exploration of women’s knowledge and experience of perimenopause and menopause: An integrative literature review. Journal of clinical nursing, 32(15-16), 4528-4540.
Pinkerton, J. V., Stovall, D. W., & Kightlinger, R. S. (2009). Advances in the treatment of menopausal symptoms. Women’s Health, 5(4), 361-384.
Pinkerton, J. V., & Stovall, D. W. (2010). Bazedoxifene when paired with conjugated estrogens is a new paradigm for treatment of postmenopausal women. Expert opinion on investigational drugs, 19(12), 1613-1621.
Polo-Kantola, P. (2011). Sleep problems in midlife and beyond. Maturitas, 68(3), 224-232.
Roth, T., Coulouvrat, C., Hajak, G., Lakoma, M. D., Sampson, N. A., Shahly, V., … & Kessler, R. C. (2011). Prevalence and perceived health associated with insomnia based on DSM-IV-TR; international statistical classification of diseases and related health problems, tenth revision; and research diagnostic criteria/international classification of sleep disorders, criteria: results from the America insomnia survey. Biological psychiatry, 69(6), 592-600.
Santen, R. J., Stuenkel, C. A., Burger, H. G., & Manson, J. E. (2014). Competency in menopause management: whither goest the internist?. Journal of women’s health, 23(4), 281-285.
Santoro, N. (2016). Perimenopause: from research to practice. Journal of women’s health, 25(4), 332-339.
Williams, R. E., Kalilani, L., DiBenedetti, D. B., Zhou, X., Fehnel, S. E., & Clark, R. V. (2007). Healthcare seeking and treatment for menopausal symptoms in the United States. Maturitas, 58(4), 348-358.
Wood, K., McCarthy, S., Pitt, H., Randle, M., & Thomas, S. L. (2025). Women’s experiences and expectations during the menopause transition: a systematic qualitative narrative review. Health Promotion International, 40(1), daaf005.
Zhu, C., Thomas, N., Arunogiri, S., & Gurvich, C. (2022). Systematic review and narrative synthesis of cognition in perimenopause: The role of risk factors and menopausal symptoms. Maturitas, 164, 76-86.
References for Behavioral Perspectives on Topics in Hormones and Behavior:
Altundağ, S., & Çalbayram, N. Ç. (2016). Teaching menstrual care skills to intellectually disabled female students. Journal of clinical nursing, 25(13-14), 1962-1968.
Ballan, M. S., & Freyer, M. B. (2017). Autism spectrum disorder, adolescence, and sexuality education: Suggested interventions for mental health professionals. Sexuality and Disability, 35, 261-273.
Barrett, R.P. Atypical behavior: Self-injury and pica. In Developmental-Behavioral Pediatrics: Evidence and Practice; Wolraich, M.L., Drotar, D.D., Dworkin, P.H., Perrin, E.C., Eds.; C.V. Mosby Co.: St. Louis, MO, USA, 2008; pp. 871–885.
Carr, E. G., Smith, C. E., Giacin, T. A., Whelan, B. M., & Pancari, J. (2003). Menstrual discomfort as a biological setting event for severe problem behavior: Assessment and intervention. American Journal on Mental Retardation, 108(2), 117-133.
Edelson, S. M. (2022). Understanding challenging behaviors in autism spectrum disorder: A multi-component, interdisciplinary model. Journal of personalized medicine, 12(7), 1127.
Gomez, M. T., Carlson, G. M., & Van Dooren, K. (2012). Practical approaches to supporting young women with intellectual disabilities and high support needs with their menstruation. Health Care for Women International, 33(8), 678-694.
Holmes, L. G., Himle, M. B., & Strassberg, D. S. (2016). Parental sexuality-related concerns for adolescents with autism spectrum disorders and average or above IQ. Research in Autism Spectrum Disorders, 21, 84-93.
Jain, N. (2024). Effect of hormonal Imbalance on mental health among young women.
Klett, L. S., & Turan, Y. (2012). Generalized effects of social stories with task analysis for teaching menstrual care to three young girls with autism. Sexuality and Disability, 30, 319-336.
Laverty, C., Oliver, C., Moss, J., Nelson, L., & Richards, C. (2020). Persistence and predictors of self-injurious behaviour in autism: a ten-year prospective cohort study. Molecular autism, 11, 1-17.
Mattson, J. M. G., Roth, M., & Sevlever, M. (2016). Personal hygiene. Behavioral health promotion and intervention in intellectual and developmental disabilities, 43-72.
Moreno, J. V. (2023). Behavioral Skills Training for Parent Implementation of a Menstrual Hygiene Task Analysis. The Chicago School of Professional Psychology.
Rajaraman, A., & Hanley, G. P. (2021). Mand compliance as a contingency controlling problem behavior: A systematic review. Journal of Applied Behavior Analysis, 54(1), 103-121.
Richman, G. S., Reiss, M. L., Bauman, K. E., & Bailey, J. S. (1984). Teaching menstrual care to mentally retarded women: Acquisition, generalization, and maintenance. Journal of Applied Behavior Analysis, 17(4), 441-451.
Rodgers, J., & Lipscombe, J. O. (2005). The nature and extent of help given to women with intellectual disabilities to manage menstruation. Journal of Intellectual and Developmental Disability, 30(1), 45-52.
Shors, T. J., Lewczyk, C., Pacynski, M., Mathew, P. R., & Pickett, J. (1998). Stages of estrous mediate the stress-induced impairment of associative learning in the female rat. Neuroreport, 9(3), 419-423.
Wegerer, M., Kerschbaum, H., Blechert, J., & Wilhelm, F. H. (2014). Low levels of estradiol are associated with elevated conditioned responding during fear extinction and with intrusive memories in daily life. Neurobiology of learning and memory, 116, 145-154.
Veazey, S. E., Valentino, A. L., Low, A. I., McElroy, A. R., & LeBlanc, L. A. (2016). Teaching feminine hygiene skills to young females with autism spectrum disorder and intellectual disability. Behavior analysis in practice, 9(2), 184-189.
References for Conclusions (Menstruation as a Vital Sign; Insulin Resistance and Hormones; Premenstrual Exacerbation)
Akturk, M., Toruner, F., Aslan, S., Altinova, A. E., Cakir, N., Elbeg, S., & Arslan, M. (2013). Circulating insulin and leptin in women with and without premenstrual disphoric disorder in the menstrual cycle. Gynecological Endocrinology, 29(5), 465-469.
Diamanti-Kandarakis, E., & Christakou, C. D. (2009). Insulin resistance in PCOS. Diagnosis and management of polycystic ovary syndrome, 35-61.
Eckstrand, K. L., Mummareddy, N., Kang, H., Cowan, R., Zhou, M., Zald, D., … & Avison, M. J. (2017). An insulin resistance associated neural correlate of impulsivity in type 2 diabetes mellitus. PLoS One, 12(12), e0189113.
Kolu, T. C. (2023). Providing buffers, solving barriers: Value-driven policies and actions that protect clients today and increase the chances of thriving tomorrow. Behavior Analysis in Practice, 1-20.
Kuehner, C., & Nayman, S. (2021). Premenstrual exacerbations of mood disorders: findings and knowledge gaps. Current psychiatry reports, 23, 1-11.
Lin, J., Nunez, C., Susser, L., & Gershengoren, L. (2024). Understanding premenstrual exacerbation: navigating the intersection of the menstrual cycle and psychiatric illnesses. Frontiers in Psychiatry, 15, 1410813.
Sullivan, M., Fernandez-Aranda, F., Camacho-Barcia, L., Harkin, A., Macrì, S., Mora-Maltas, B., … & Glennon, J. C. (2023). Insulin and disorders of behavioural flexibility. Neuroscience & biobehavioral reviews, 150, 105169.
Ueno, A., Yoshida, T., Yamamoto, Y., & Hayashi, K. (2022). Successful control of menstrual cycle‐related exacerbation of inflammatory arthritis with GnRH agonist with add‐back therapy in a patient with rheumatoid arthritis. Journal of Obstetrics and Gynaecology Research, 48(7), 2005-2009.
Vollmar, A. K. R., Mahalingaiah, S., & Jukic, A. M. (2024). The Menstrual Cycle as a Vital Sign: a comprehensive review. F&S Reviews, 100081.
Yu, W., Zhou, G., Fan, B., Gao, C., Li, C., Wei, M., … & Zhang, T. (2022). Temporal sequence of blood lipids and insulin resistance in perimenopausal women: the study of women’s health across the nation. BMJ Open Diabetes Research & Care, 10(2).
These days, I’m thinking in terms of permaculture and sustainability. So when I feel like complaining that a beautiful, unique variety of plant would come thrive in my environment but IS NOT HERE, I can’t sit around wondering why it doesn’t come, without doing some work.
What are its requirements? What does it need in the soil? Are there some things in my soil, or the biome, or the other plants thriving here, that are actively repelling it? Is it perfectly happy where it is? Do I want it because it would beautify MY surroundings, or for reasons that mutually benefit us all?
I have seen several types of posts on social media responding to the article that came out on keynote speaker trends. Each of these reaction posts includes voices that count, and many of them would not have been heard if we only read peer reviewed publications. There have been personal responses to the topic; discussions of the current state of injustice; brainstorming on why the problem exists and ideas about better metrics to use. What about actionable suggestions by academics ourselves?
Note that I barely count in this regard; one of my dissertation advisors cautioned me, “once you get out of academia good luck getting back in” as I pondered a position providing behavior analysis across the lifespan with people on Medicaid waivers and diverse genetic diagnoses. But I’m glad I didn’t listen, because my life has been richer given that diverse clientele who taught me so much across hospitals, nursing homes, and their vocational sites. That is mine to keep although I had very little time (and sometimes not enough discretionary money) to publish (and no backing institution). However, I still held (and still hold) certain privileges and advantages as a white, Ph.D. level person with certification.
So instead of a treatise on my personal feelings, my thoughts on who I would like to hear from at conferences, or ideas for a better more inclusive metric on who should be selected, here are actionable items for others.
Treat this as a call-in and focus on what we can do about it, since we (e.g., the people with academic degrees, histories, and/or publishing experience) have a pivotal role in changing the landscape. (Thanks Paulie Gloves for the idea on how to treat this opportunity). I think the question is whether we actually want to. If you do, here are my 10 suggestions.
2. As we acknowledge our advisors and labs when presenting, acknowledge also the people who inspired our ideas, who informed the work, and provide examples of ways to support it and them.
When given invitations to present or speak, ask ourselves how we could and whether we should platform others. Some of the ways I have done this include:
3. When being asked to speak on a topic, consider someone else who may be much less known but whose expertise and lived experience would be valuable to the listeners. Whether the venue selects the person I point out is up to them, but I can put them on someone else’s radar.
4. When asked to speak, invite someone on the platform with you.
5. When asked by a journal editor for suggestions on people to review an article, consider perspectives that would be important and overlooked. (But be transparent; being invited may add to someone’s burden of time and it is unpaid labor others may not have the luxury to accept. I invite anyway, because I do not want to ASSUME someone’s circumstances and presume I KNOW whether they would or would not want or be able to prioritize such labor and experience.)
6. Consider whether you could be a part of creating platforms (like topic-driven conferences that honor diversity and lived experience, that are not bound by the rules other organization-driven opportunities are). There are several wonderful examples of these.
7. If you attend one of those experience-driven conferences and are inspired, consider calling in the speakers who would not have otherwise been able to publish, and see whether this kind of work is a goal of theirs. Provide opportunities for collaborative writing if they are interested.
8. When paid for speaking that only you could have done, consider whether your fees could go back to the community you are trying to help, or work with a financial advisor to create such a path for some of your fees.
9. In systems (as company owners), please wait to get into the business until you can afford to fully staff your clients to the extent that your staff can (a) prioritize actions aligning with their values, and (b) stay healthy and buffered themselves. If they are overworked they will never have time to attend a conference, present a poster, participate on writing an article, or explore their ideas about a topic they learned and want to apply in meaningful ways to your shared clients.
10: Amplify others’ messages in your own circles. There may be a temptation to agree in public but behind closed doors, to continue to engage in the lower-cost actions that perpetuate the system as is. If we really wanted to see and live in a different landscape in 10 years, what would it take for you to do THIS YEAR to nudge those shifts?
What’s next? those of you who have served in additional capacities on editorial boards, performed roles in companies, and published extensively know that there is more to the story and you have additional suggestions that would make an impact. I know you do. Let’s hear them.
Why are values meaningless without contextual understanding, and committed action? And what’s the connection to Homer Simpson?
The question is found in both behavioral and permaculture applications. If you caught my talk at Stone Soup ABA 2024 sponsored by Lake Ridge Community Support Services, you heard a permaculture example (e.g., the seemingly value-based statement “if you value native plants, root out all invasive species”). This loosely parallels the concept of “just ignore junk behavior and reinforce what you DO want” in behavior analysis.
Is it always best to rip out non-native plants? For behaviorists, is it always appropriate to ignore and let “junk behavior” wither and die?
Maybe part of the problem is our misuse of the concept of “always”.
Now, I was fortunate to grow up with a witty, smart as a whip, biologist mom. She cared about the earth (more than my teen feelings of embarrassment, which I outgrew thanks to her bold example) and called out high school boys who littered right in front of her. She took us to Earth Day events even when we were one of the only families there (and, consequently, I WON the Earth Day Fishing Tournament, having been the ONLY entrant in my class). She wore the same Big Bend hat for decades, was a master gardener and a proud member of our local Native Plants Society, and championed native plants.
But she evolved with knowledge, like a true scientist does, and she would value the principles of permaculture that I’m learning about now.
Do we need to remove this thing, or understand it first?
For example, now we ask questions before we pull things out. Why is this plant here? Why does it grow, when almost nothing else is growing? What special features does it have that makes it thrive in a barren space of edges where the beautiful native plants we wish were here… AREN’T?
We appreciate the many interlocking functions of the thing we observe before us. What is it doing for the soil? Is it taking up space and time in an important way, holding the soil in place where it would have eroded due to habitat loss faced by the native plants leaving? Is it providing habitat for insects, birds, shade loving plants or others who need it?
If I say my value involves loving native plants but I mindlessly remove non-natives without considering THEIR roles too, I risk failing both natives and non-natives.
OK… what’s that got to do with Homer Simpson? Well, look. I want you all to be able to use the buffers. And one exercise I provide to teams or families new to them, is a little fun challenge: see how many you can use today. Why, go ahead and think about a single HOUR. How many can you use? For instance, Homer is… eating a sandwich (nutrition(ish) buffer)… while in bed… (sleep buffer?) with Marge (relationship buffer)… maybe this is helping his mental health and stress relief. Maybe they’re going to get in some exercise later this evening.
But here’s the thing. You need values, AND you need inter-relatedness among the buffers. We care about intentional connections, not simply combinations.
Homer’s always missed something. He loves Marge, but he often doesn’t think about her experience at all. He’s getting some buffers in, sure, but you know what happens almost immediately in this episode?
“Marge, I’d like to be alone with the sandwich for a moment.”
When we’re self-serving with our buffers, or mindlessly try to “get them all in” (or put them on someone else’s schedule when they haven’t provided their assent (see the BACB Ethics Code and its descriptions of it or learn more here) or even their INPUT), we’re not really embodying that value of fostering interconnected buffers.
Something I recommend is picking a buffer that guides your others… and anchoring committed actions to the OTHER buffers that reflect back that first one. (Interested in this? Work with or care about teens? Check out The Thriving Adolescent, for concrete suggestions and examples around selecting a value and identifying committed actions that reflect those.) For those of us in relationships, maybe it’s the idea that most of all, you want to value and protect the nurturing relationship. Then the other buffers can be designed around actions that reflect this. I know when I do this, I eat well because I’m making loving healthy meals for and with all my family members and we’re eating together. So, my nourishment is enmeshed with theirs and I’m no longer skipping meals, angrily lashing out because I’m hungry or protein deficient, or angry about having to come up with yet another meal idea. I could write a paragraph about each buffer and how it can all relate back to the nurturing relationship I want to foster with my close family members.
When Junk Isn’t Necessarily Junk
What does this have to do with junk behavior? Well, just like non-native plants wouldn’t be there if natives were all thriving. When the environment fosters the conditions which give rise to a healthy balance between plants, people, animals, insects, and the land, it works. And you can often think of many features of so-called “junk” that make it useful for someone else!
When something is rooted out… to make space for development, or there’s a huge loss of a predator, or an introduction of a new animal, etc… other things wander in. Before you trash them, notice them. Maybe they’re playing a role you need to notice, watch a while, understand.
When we change behavior with a plan, a transition, a death, whatever intentional or unintentional changes occur… other things wander in. So often we look only at how we can yank it OUT, without considering why it’s there, what purpose it’s serving. In the terms of buffers, is it temporarily helping someone to tolerate distress? To eat when there’s nothing else? To get rest or escape from their aversive environment? To take up space in their repertoire because there is a lack of meaningful things for them to do, see, say, hear, etc?
Someone wouldn’t use a whole lot of “junk behavior” if their needs were being met, they had tons of skills to communicate effectively, they had meaningful things to do all day and loving listeners to help them spend their time with purpose. (Look at this beautiful way to meet needs WITH “junk” instead of wasting it, and buying yet more building materials!)
The Next Step
Anyway, I hope you enjoy thinking about the buffers today and remembering it’s up to you to do all three: identify your values, understand your context, and design meaningful, committed actions that get you closer to those values. One step closer is enough today. Maybe your step is picking the buffer that most aligns with your core values and operationalizing that one right now! 😊
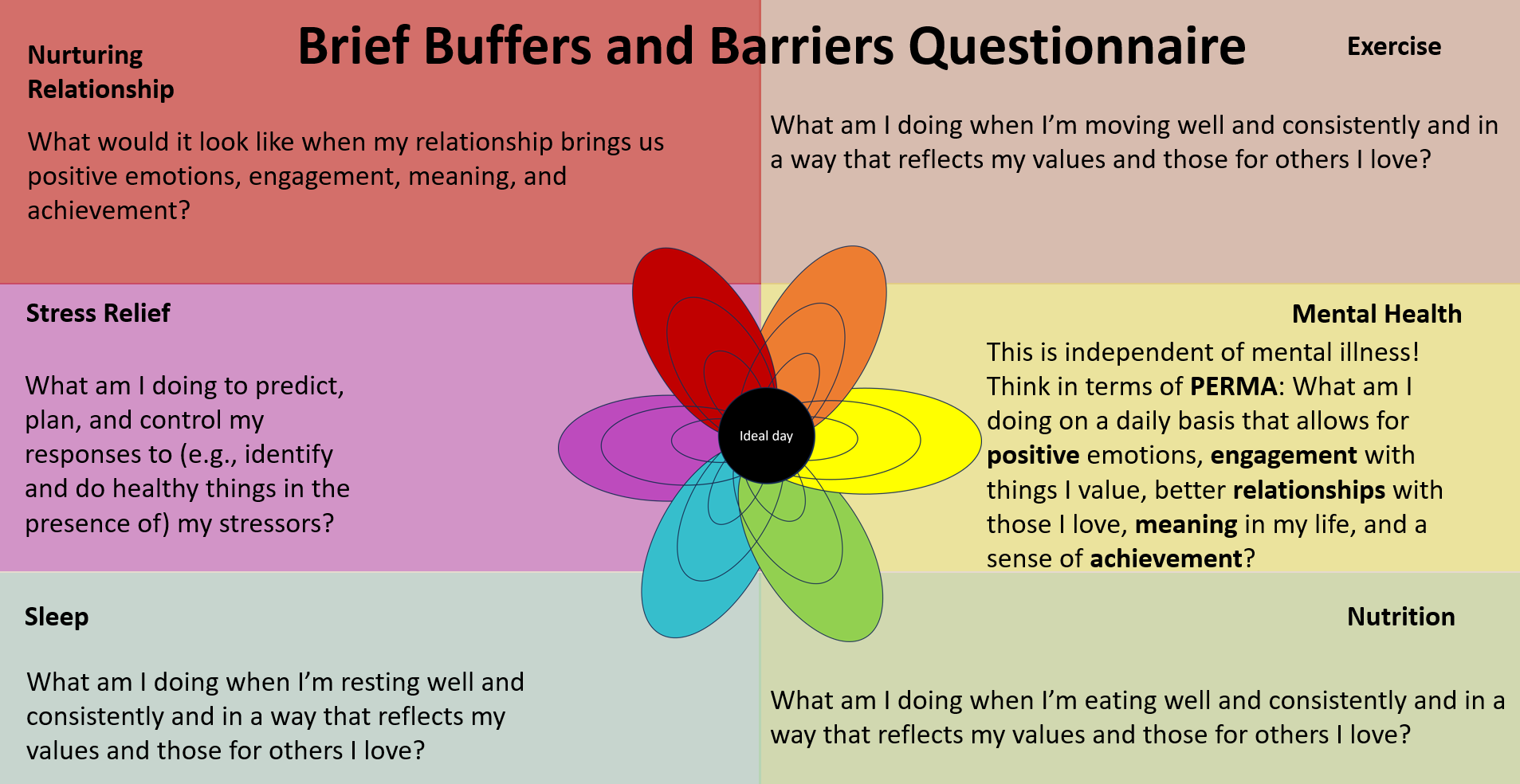
Ready to take Today’s Next Step? Pick ONE buffer below and operationalize it. That means, jot down what it would look like for you to engage in things that reflect your values in this area. What would you wake up and do, and do throughout the day, if your actions in this buffer area really reflected your values?
Another article in the trauma-informed series by Dr. Teresa Camille Kolu, Ph.D., BCBA-D
In relationships we do rituals.
“BLECH!” Startled, I looked down at my sweet, expressive daughter with a true disgust face. Everybody laughed. I was kinda mortified but I laughed too. The woman at MeOhMyCoffeeAndPie (you HAVE to go) had just answered her question with “it’s sauteed onion” when my kid asked “what’s the scone flavor today?”
Ok, I guess she wasn’t expecting that.
I was too caught up noticing this awesome tiny, framed quote by the display case. As a young reader I LOVED Larry McMurtry, see, who wrote Lonesome Dove and a whole lot more. He and I both went to UNT (decades apart, of course) where he gave us a wonderful author meet and greet (early 90s for me, when this kid was not even a twinkle). The coffee and pie shop had quite appropriately chosen to frame this gem of a quote: “She made great biscuits, but her behavior was TERRIBLE”.
My daughter and I were out doing a ritual Saturday thing. My mom used to sing “Come Saturday Morning” with me (we had the sheet music, so it was right up there with “Country Roads” and “The City of New Orleans” in my book). And sometimes we would spend time just us, and I would look at her hands and sing this song in my head. Saturday mornings, for a couple precious hours, are time when my daughter doesn’t have to share me with her little brother, and she pays me back by asking me questions I can’t answer. It’s at this time I learn that even 5 year olds wonder things about God and the universe, have nightmares, they can have crushes, they have fears, they might still want to hold my hand.
I LOVE biscuits but I love her even more. I love her more than her behavior, even that sort of behavior that makes you want to fire the babysitter just so you’ll never have to greet that face that saw the terrible behavior you thought your kid would never do in public and after all, you are a behavior analyst! (Do I think it’s easier because I’m a behavior analyst, my new friend asked recently? Heck no. I personally think it’s harder. But I do think being a parent has made me a better behavior analyst.)
So in relationships we do rituals, like setting up meaningful goodbyes when we leave the room, or when rhythms change and we won’t be spending as much time together anymore. If not, we leave devastation.
When I watch animals grieving each other’s deaths… especially horses and dogs… I notice how fully present they are for the goodbye.
And I am always grieved to consider the implication: such a meaningless slog of goodbyes without reason, or participation, we inflect this on clients when caseloads shift; when a therapist moves; when a client with certain behaviors moves into Hall B, so we just HAVE to abruptly move Client A into Hall D, so they won’t antagonize each other and never mind Client A will never again see her best friend client, or even the janitor—who was like a mother to her and had been there for 12 of the client’s 15 years in this mental facility again.
We often have to make hard decisions, but we should ask questions (“what really hurt your feelings this past week? Today?”) because in relationships we apologize when we’re wrong.
When we realize we hurt others, we shift so that we won’t keep doing the hurtful thing.
My mom remembered the pain of being hurried as a child. I knew that, and I forgot it. I remembered it again this month when I was going through an exercise I was making for a new workshop we will offer at cuspemergenceuniversity.com. The exercise has us grownups go through questions that reveal the triggers for us – the things in our everyday situations that make us more likely to react swiftly (often in a hurtful way) to the others around us. And I realized two things: being hurried doesn’t feel good to children, and hurrying children doesn’t feel good to adults. So what do we do? This week, maybe you will notice a ritual that is always done with urgency, and think, how does this feel? What would this feel like if I slowed down? Now, the harder part: What would it take for me to build in space around this… ten extra minutes before it, so that we don’t have to experience this, every single time, in hurried mode? I tried this, and my children really love it, although I won’t hear about it from them. Their lingering hugs (mama, don’t let go first!) and their wonder as we have time to look around the yard for a new flower before we buckle our seatbelts… the absence of urgent reminders and exasperated sighs… perhaps even a reduction in tense moments when I’m about to lose it and yell. These changes are rewarding enough for me to keep doing this. Because I love them more than biscuits.
Yes, rapport is often transactional. Although it was by design at first, it doesn’t always have to be that way. I talk about this just a little bit in my buffers article, in the relationship section. And in the trauma sensitivity course we talk a little about how to be more sensitive to what folks go through (including your staff) so that YOU can be a little less harsh, a little more supportive, around things you didn’t even realize were hurting the other person.
In relationships, we apologize; we give freely; we do things uncontingently (yes, I know you won’t be able to look that up, and there’s a reason- we talk about it more on instagram and it bears more attention); and we are generous with things the person really needs, like time, kind words, and those little rituals that they consider special. Have you ever worked with a therapist the client really adored? Or a professor beloved by their students? I remember two. The professor is loved and really loves. She gives generously of her wisdom, time, and appreciation for students. (You wanted to ace her class and reflect what you admired in her, even as she whispered the things that made you more of yourself, more creative and passionate and able to grow confidently in the direction of your dreams.) The other person I remember is a therapist who had kids riding on her shoulder at recess in our mixed school for kids with developmental differences and peers. And those folks taught me that you can have instructional control when it’s time, and still have fun with the people who look up to you. Rapport IS often transactional. But the relationship doesn’t have to be.
Thanks for reading.
Oh… and I personally think, in the Longmont area, that Lucille’s has the best biscuits.
And OhMeOhMyCoffeeAndPie has the best lemon bars, if you’re wondering.
I love you more than biscuits, daughter of mine. And I love you even when your behavior is terrible.
Another article in the TIBA series by Dr. Teresa Camille Kolu BCBA-D
In Chapter 8 of our course on Trauma Sensitivity, we cover the concept of “triggers” and what we can do about them. We cover this mostly from a responsive perspective in the course and use the following operational definition: “Triggers are historically meaningful stimulus complexes or relations between them. In their presence, behaviors or response patterns may be temporarily more likely to occur.” We continue with the big idea from Chapter 8 of that course, “One of the most supportive actions we can take is to stay mindful and do what needs doing in the moment”.
However, another huge thing we can do in helping someone through those triggering events or moments is to plan ahead. Below are some questions we ask our clients and their family members to answer, if they are interested in exploring this. Read on if you’re interested in some examples (we share a brief example of a dyad’s answers, where one member is the 5 year old kid, and the other is a parent). (Oh, and it may be helpful to check out the IPASS (find it in our RESOURCES tab)- this is a little tool we use for folks to go through their sensory environment for clues about triggers, if they need somewhere to start.)
Questions:
1.Name a person you love or a primary relationship you care deeply about.
2.Name an action that you do that shows compassion with them.
3.Name some things the person also does… that REALLY get under your skin.
4.Name an environmental situation or trigger that happens right before it is HARDEST to keep your cool.
5.List some things you start to notice when you’re feeling about to blow up/ lose your cool/ start doing actions that are inconsistent with your values to that #1 person.
6.State things you do to calm down in those moments that REALLY work or are most likely to work.
7.If you DIDN’T act to calm down and things kept getting worse, state the action(s) you would be likely to use next in the presence of that person.
Growth statement: Write your plan to prevent the triggers (3 and 4 above) from leading to actions that are inconsistent with your values (e.g., 7), by doing (6) as soon as you begin to notice things about your insides or the outside environment (5).
Ready to see this in action? Below are some parent answers. Keep in mind that neurodivergent parents often have neurodivergent children (or, looking backward, that neurodivergent children often have neurodivergent parents, whose qualities might not be appreciated until later, in the context of exploring diagnoses with their own children). Have you ever seen a mom struggling with her own misophonia exactly at the same time her child uses loud repetitive noises? Talk about triggering (for and to each other)! But stay hopeful and in the moment, because as hard as it is to be the thing in your loved one’s environment that sets them off, it’s lovely to be the person in their environment who can really understand where they’re coming from.
Parent Example: Answers to 7 questions, above
1.I love my kids.
2.I love it when I am able to use kind words and a calm voice with them.
3.Sometimes my kid makes repetitive noises, does not listen or interrupts me, or doesn’t follow instructions.
4.It is most difficult to keep my cool with my kids when I’m running late somewhere and my kid is not following instructions or is not doing something the “right” way.
5.I start to notice my face getting hot, my neck and face muscles are strained, and my breathing is shallow and fast.
6.If I splash water on my face, relax my muscles, stop and hug my kid, and breathe deeply, it helps to calm me down in the moment.
7.If I skip that step above, I usually proceed to raise my voice and may even shout or say things I don’t mean (things that are not kind and compassionate).
Parent Growth plan: “When I’m late somewhere and it’s really noisy, it’s especially important that I start to notice when I’m using shallow breath, the noise around me is increasing, or I’m noticing everything “wrong” my kids do and nothing right they’re doing. Right then, before I talk to my kid, I need to immediately try some of my calming strategies I listed above.”
OK, now for the kid’s answers.
1.I love my mom and baby brother.
2.I love it when I am able to keep playing, share, have fun.
3.Sometimes my mom tells me to stop doing something I love or tells me how to do something better or my brother takes my stuff.
4.When mom yells or my brother takes my stuff or we have to leave my game or book, it is most difficult to keep my cool.
5.I start to notice my face getting hot, my movements are jerky, my chest hurts, and my breathing is fast.
6.If I hug my mom, splash water on my face, stop and do some jumping jacks and then sit and breathe, it helps to calm me down in the moment.
7.If I skip that step above, I usually yell, hit my brother, or shout “NO! I WON’T!”.
Growth plan my parents can help with: When I’m being asked to stop playing or to do something that interrupts my flow, notice when I’m breathing faster and having a hard time talking. You can help by giving me a hug, doing some jumping jacks with me, and sitting with me and helping me to breathe.
At this point, we ask the parent some meaningful questions to help them make sense of what we’re noticing. And often this is uncomfortable (but becomes exciting and doable) as they first think, “oh, but won’t we be reinforcing escalation?” No, we’re turning it off.
Parents or caregivers, did you notice…
-Whether your having a hard time makes it harder for you to help your other person with THEIR hard time?
-Whether your hard time perhaps CONTRIBUTES to their hard time?
-Whether your triggers are echoed by the ones that seem to affect your kid or client? (e.g., are you teaching your other person to struggle with the same thing you struggle with, without your meaning for this to happen)?
-Whether your triggers might be easier to manage at a period of time when you (or both of you) are well fed, rested, and exercised?
Specific buffers (see Purewal et al., 2016) can actually protect against the harmful impacts of ACES on medical health. The particular buffers found to reduce harm include getting enough sleep, eating nutritious food, having access to mental health care, experiencing a safe relationship with someone, exercising regularly, and practicing stress relief techniques that allow someone to experience calming down (such as a simple mindfulness technique). Adding buffers may be a set of seemingly small actions, but they contribute to preventing problems from becoming larger, and may help solve challenges related to why a behavior plan is just not working. (Solving basic problems in the behavioral environment regarding access to needs can be an area consistent with the ethical imperative behavior analysts have to address conditions interfering with service delivery; see BACB, 2020, 2.19).
Although the buffers make a big difference in preventing from harms and protecting against future ones related to ACES, many individuals and families face major barriers related to access, information, resources, or behavioral needs. These barriers can reflect resource inequalities, individual differences, and cultural challenges that prevent many from experiencing the benefits. How could we leverage “buffers and barriers” policies to protect against harms (and truly embody the preventative arm of behavior analysis)?
One of the difficulties with beginning to implement buffers for individual clients is that behavior analysts may be hesitant to devote precious resources to this new and potential preventive area. To assist teams in understanding further how policies might affect our clients, their caregivers, and our staff, Cusp Emergence is engaged in developing resources and collecting feedback about their use. Some of the resources provide examples for conversations we could have with others, while others are visuals to help others easily understand the buffers and barriers (such as the “Be a buffer. Solve a barrier” downloadable pdfs in this article). We also have lists of policy ideas for interested agencies, risk benefit assessments to aid in their implementation, and examples of how we define buffers for individual clients, families and staff. Use our contact us form below to let us know which resources are your favorites or what else would help you more actively approach this area. Oh, and stay tuned for more on this incredible topic. Soon we’ll be be exploring buffers in more detail, including sharing some ways we integrate it for our clients, how it can be meaningful for caregivers and staff, and some of the research on each one.
For me, an on-demand workshop does several things: It can be taken any time; one can take it with a group and apply exercises with other people if desired; but since it’s on-demand, an individual will benefit even if taking it solo. It should be expandable if one wants to be able to sit with a chapter for a few extra hours because we simply love the content; there will be resources to grow with and come back to if one can’t do all the exercises right NOW. I’ve been on sabbatical a while; as I return to doing interviews, conferences, talks, and podcasts (including a new one we taped recently for the Atypical Behavior Analyst, with my friend Dr. Eddie Fernandez airing later), it is nice to be able to take something on my own time, when tiny folks are asleep, and I know many parents – and folks going through school and work at the same time – are in the same boat.
30+ exercises with the videos: Because this is an on-demand workshop, we present a TON of exercises packaged with the videos. Teams or individuals can easily do a chapter a week along with exercises for a truly transformative experience in your office or supervision setting. But if they choose to take it all at once in an afternoon, that’s possible too. So it’s customizable.
Scalable applications for team members, supervisors and supervisees: The new content (on leveling up the trauma sensitivity of our staff and client environments) is “scalable”, meaning we include applications for 3 different levels of staff: those in roles that are basic; intermediate; and advanced. Presenting it as a workshop meant that the team members “leading” the discussions and exercises benefit just as much as (but different from) the less advanced team members they are mentoring through it.
Supervision guides and chapter handouts: These come with every chapter video and walk the student through the material, from the main ideas we presented, to definitions for any new vocabulary, exercises, lists of Ethics Code items that relate, thoughtful discussion questions, exercises, and chapter resources and articles. Every chapter comes with its own handout and supervision guide to help BACB supervisors or team leaders support our coworkers and supervisees.
The two things I personally love most about this workshop are:
it addresses tough topics like moral injury with your team members and considering how this ethics area could apply to our supervisees but our clients too;
and we provide resources to follow up on big ideas like this one: there are some behavioral needs that medical providers consider symptoms of trauma-related concerns. (If folks are new to integrating trauma sensitivity in their supervision and client environments, we might miss this huge opportunity to make sure we do no harm by treating behavior needs that are actually related to new abuse.)
Wondering about the content of the new workshop? Here are the chapters (each has its own video, ethics intersections, resources, thought questions, and exercises):
Chapter 1: Principles of Trauma-Sensitive Care
Chapter 2: Interactions that could help or do harm
Chapter 3: Features of trauma-related responding
Chapter 4: Defining trauma
Chapter 5: Risks related to trauma
Chapter 6: Elements of a potentially trauma-related response
Chapter 10: Want to mitigate risk? Document it first
Chapter 11: Skills and Stress
Chapter 12: Healthy Collaboration
Above: Table of chapters from Trauma Sensitivity in the Behavioral Workplace, new on-demand workshop from Cusp Emergence
Did you enjoy this article? Come back soon when we’ll cover a few more related topics including: mentorship groups for those applying trauma sensitivity principles in their supervision sessions; how to get the most out of your workshop experience by doing exercises as a group or dyad; more info on a brand new all-trauma conference coming in April hosted by the formidable Dr. Gabi Morgan; meetups in Denver May 2023; and more!
Read below for final thoughts and some links if you’re in the market for values related CEUs: Recently, when my own CEU cycle was about to turn over, I knew it was time to take a course or workshop in something I could use NOW and am passionate about… so I went searching for three things: supervision CEUs; offerings from people I admire and from folks who literally wrote the books on leveling up mentorship and supervision and working with families; and opportunities to learn about values in a deeper way that would help me level up my own practice. That led me to a couple of great courses and podcasts; one of these opportunities was a workshop with built in exercises that could be taken quickly or over the course of a few weeks and included opportunities to network with other folks. It was a really lovely experience. Included are links to a couple trainings and podcasts from respected folks who continue to inspire, below.
Have you heard of the Stone Soup Conference? I’m so proud to join a group of amazing presenters to share lessons and ideas with folks in the behavior analysis community. All proceeds go to Lake Ridge Community Support Services, and (in their words) “build capacity to provide applied behaviour analysis services to children, youth and their families who are in financial need and waiting on service through the ABA for All Fund”. That’s a pretty great mission and I’ve worked with them before… this organization was one of the “early adopters” of anything trauma-related! Years before anyone wanted a keynote about trauma, these folks were simply interested in helping their practitioners get mentorship and consultation for “tough clients” struggling with their returns to communities. I think this type of consultation helps newer practitioners, and ones whose existing clients grapple with new challenges, to fulfill this piece of our Ethics code: “Being aware of, working within, and continually evaluating the boundaries of their competence” (Ethics Code for Behavior Analysts, p. 4).
That’s why I was so eager to say “yes!” to this invitation (and thanks so much for our connection, Matt! Your podcast continues to bring exciting topics to forge new paths for behavior analysts interested in growing our repertoires… like exposing us to Rajamaran’s article (finally!) putting trauma in the pages of JABA where it belongs. I loved hearing the stories behind it).
So next week, join me as I talk about horses and love and most of all, why I believe it’s so important to honor the SPIRIT in addition to the LETTER of the Ethics Code: You will find “Treat Others with Compassion, Dignity, and Respect” on page 4, but you will not be able to find a specific code number about it. That might make it seem like it’s not as worthy of an ethical goal. However, it’s actually such an important idea that it pervades and breathes life into every single other component of the Code.
More on this during my talk next Friday. If you can, join us. Check out my teaser video here, then check out other folks’. Come for the CEUs and stay for the stories. I can’t wait to see you in the virtual space!
Last time I wrote, I shared some ideas about this intersection. Today, the new course is up! Before you go check it out (and claim your February 2022 coupon for 20% off by typing ASD2022)– during the introductory month of the course)- learn why I’m so passionate about screening for trauma in a population so many behavior analysts have been working with (for some, virtually their entire professional lives).
Have you ever worked with someone in pain? How do we know if they’re currently hurting, whether it’s because they are sick, it’s related to interventions we chose, or from experiences we reminded them of? How would we know if that was the case? Did that person cower, freeze, or grimace? Did they flinch, close their eyes, seem to “zone out”? Perhaps someone has run away, played repetitively with the toys they had, or fallen asleep at school? Sometimes, respondent behaviors may be giveaways that people are experiencing fear or in pain, but successful avoidance behavior can hide that pain. Other times people have been through experiences making them more likely to use aggression or property destruction. In the least, we should consider whether our interventions cause harm. This harm could include causing our clients distress or pain, exposing someone to additional risks, detracting from their quality of life, failing to program in sustainable ways that transfer to the maintaining environment, and so much more.
A new training is up on Cusp.University on the intersection of autism, trauma informed behavior analysis, and ethics. By the time we near the end, we have discussed and revisited the idea of contra-indicated procedures. Given that lists exist for diagnoses of autism alone, why isn’t there a list of best practices appropriate for clientele meeting diagnostic criteria for autism who also come to therapy with trauma histories? Why is it so difficult to find articles suggesting best treatment paths for individuals with both autism and trauma related experiences in the literature? In behavior analysis, answers to these questions may be related to our field, its historical publishing practices, and the ethical and pragmatic need to individualize procedures for each client.
In terms of publishing practices, a panelist in ABAI’s “Exploring Publication Bias in Behavior Analytic Research” (which included Galizio, Travers, and Ringdahl, 2021) stated,
“No intervention is guaranteed to work for every individual, every time, in every context.”
They suggested that authors writing about their research should include more detailed descriptions of the conditions under which successful implementation of the intervention occurred.
When we screen for trauma related or aversive historical situations and stimuli, we often learn things that
help us prioritize treatment,
document risks for certain procedures,
avoid or prioritize certain stimuli,
detect environmental conditions that are acting as motivational operations and conditioned MOs,
and ultimately, perhaps minimize harm to our client.
Screening for trauma can help to identify individuals with prior risk factors who are at risk for experiencing additional adverse events and aversive conditioning. Attendees learn in chapter 1 some facts about how being autistic is to be at increased risk for trauma, bullying, abuse, increased likelihood of experiencing foster care—and in chapter 3, learn about the higher rates of experiencing restraint, seclusion and being excluded from school.
But another effect of screening – one that should affect all behavior analysts—could be an increased awareness of the fact that behavior analytic procedures are being used all the time for this population at the intersection of autism and trauma. Perhaps the least we can do is to begin doing behavior analysis with people instead of to people, and to be transparent, inviting, and open in looking at options—and their likelihood of causing harm either now in the future.
Let’s look at this juxtaposition: we have a great ethical responsibility to do no harm, but also an ability to cause great harm. With using any behavioral procedure there comes a risk that we may do just that. This is especially true when we don’t have literature evidence that a given intervention is appropriate and effective for the person’s needs given their history and current situation. Perhaps they don’t actually need behavior analysis seeking to change their behavior as much as they need a roof, a meal, a bus pass, a blender, a respite provider, a ride to the doctor, a coat, a medication, a trip to the dentist… the list could go on and on. So clearly the first step is to see what the person needs.
When designing an individualized behavior support plan, two things are important to consider:
(1) the risks and benefits for the client themselves, given their needs, values, environment, etc., (e.g., the long- and short-term outcomes of procedures and decisions, and
(2) evidence the procedure is appropriate for our client.
In terms of evidence, when considering decisions in context of the literature, few studies provide sufficient detail in characteristics of the participants. So it is difficult to tell, reminds the panel, which characteristics were present for study participants received successful or unsuccessful interventions. Thus we can’t really tell how many of the massive number of papers on treating behaviors in autism, also apply and were conducted with individuals with autism who also had a trauma background. But statistics suggest many of them must have. In the science of behavior analysis, each subject’s behavior is its own control, so if we control our conditions and try to measure well, we may reveal additional elements of historical and current behavioral environments that exert contextual and stimulus control on the client’s behavior- and that change their needs. At times, historical aversive conditioning experiences may have contributed changes making it painful or inappropriate for clients to experience certain interventions. As we discuss in the new training, some of those conditioning experiences may even have occurred during and as part of behavioral treatment.
We can’t know for sure what our clients have been through. But when owe it to them to honor those experiences if they are comfortable sharing them.
Here are some of the things you’ll learn.
Course Objectives:
1. List connections between autism and trauma in the research
2. State different kinds or examples of trauma that may affect individuals with autism
3. State supportive ways to ask about trauma histories
4. Select examples of how medical history can be related to trauma
5. State examples of repertoires beneficial for practitioners who serve clients affected by both autism and trauma
Ready to learn more? The new training offers hints from Dr. Kolu on how we begin the conversation about informed consent and screening for trauma, why assent is so important, how trauma and autism might intersect with medical needs affecting our clients, and more. And all the resources are available as free content in the preview section, so go grab that now! See you at a conference soon or find us online. And thank you for listening!














{kind=link}
{kind=link}
{kind=link}