Why are values meaningless without contextual understanding, and committed action? And what’s the connection to Homer Simpson?
The question is found in both behavioral and permaculture applications. If you caught my talk at Stone Soup ABA 2024 sponsored by Lake Ridge Community Support Services, you heard a permaculture example (e.g., the seemingly value-based statement “if you value native plants, root out all invasive species”). This loosely parallels the concept of “just ignore junk behavior and reinforce what you DO want” in behavior analysis.
Is it always best to rip out non-native plants? For behaviorists, is it always appropriate to ignore and let “junk behavior” wither and die?
Maybe part of the problem is our misuse of the concept of “always”.
Now, I was fortunate to grow up with a witty, smart as a whip, biologist mom. She cared about the earth (more than my teen feelings of embarrassment, which I outgrew thanks to her bold example) and called out high school boys who littered right in front of her. She took us to Earth Day events even when we were one of the only families there (and, consequently, I WON the Earth Day Fishing Tournament, having been the ONLY entrant in my class). She wore the same Big Bend hat for decades, was a master gardener and a proud member of our local Native Plants Society, and championed native plants.
But she evolved with knowledge, like a true scientist does, and she would value the principles of permaculture that I’m learning about now.
Do we need to remove this thing, or understand it first?
For example, now we ask questions before we pull things out. Why is this plant here? Why does it grow, when almost nothing else is growing? What special features does it have that makes it thrive in a barren space of edges where the beautiful native plants we wish were here… AREN’T?
We appreciate the many interlocking functions of the thing we observe before us. What is it doing for the soil? Is it taking up space and time in an important way, holding the soil in place where it would have eroded due to habitat loss faced by the native plants leaving? Is it providing habitat for insects, birds, shade loving plants or others who need it?
If I say my value involves loving native plants but I mindlessly remove non-natives without considering THEIR roles too, I risk failing both natives and non-natives.
OK… what’s that got to do with Homer Simpson? Well, look. I want you all to be able to use the buffers. And one exercise I provide to teams or families new to them, is a little fun challenge: see how many you can use today. Why, go ahead and think about a single HOUR. How many can you use? For instance, Homer is… eating a sandwich (nutrition(ish) buffer)… while in bed… (sleep buffer?) with Marge (relationship buffer)… maybe this is helping his mental health and stress relief. Maybe they’re going to get in some exercise later this evening.
But here’s the thing. You need values, AND you need inter-relatedness among the buffers. We care about intentional connections, not simply combinations.
Homer’s always missed something. He loves Marge, but he often doesn’t think about her experience at all. He’s getting some buffers in, sure, but you know what happens almost immediately in this episode?
“Marge, I’d like to be alone with the sandwich for a moment.”
When we’re self-serving with our buffers, or mindlessly try to “get them all in” (or put them on someone else’s schedule when they haven’t provided their assent (see the BACB Ethics Code and its descriptions of it or learn more here) or even their INPUT), we’re not really embodying that value of fostering interconnected buffers.
Something I recommend is picking a buffer that guides your others… and anchoring committed actions to the OTHER buffers that reflect back that first one. (Interested in this? Work with or care about teens? Check out The Thriving Adolescent, for concrete suggestions and examples around selecting a value and identifying committed actions that reflect those.) For those of us in relationships, maybe it’s the idea that most of all, you want to value and protect the nurturing relationship. Then the other buffers can be designed around actions that reflect this. I know when I do this, I eat well because I’m making loving healthy meals for and with all my family members and we’re eating together. So, my nourishment is enmeshed with theirs and I’m no longer skipping meals, angrily lashing out because I’m hungry or protein deficient, or angry about having to come up with yet another meal idea. I could write a paragraph about each buffer and how it can all relate back to the nurturing relationship I want to foster with my close family members.
When Junk Isn’t Necessarily Junk
What does this have to do with junk behavior? Well, just like non-native plants wouldn’t be there if natives were all thriving. When the environment fosters the conditions which give rise to a healthy balance between plants, people, animals, insects, and the land, it works. And you can often think of many features of so-called “junk” that make it useful for someone else!
When something is rooted out… to make space for development, or there’s a huge loss of a predator, or an introduction of a new animal, etc… other things wander in. Before you trash them, notice them. Maybe they’re playing a role you need to notice, watch a while, understand.
When we change behavior with a plan, a transition, a death, whatever intentional or unintentional changes occur… other things wander in. So often we look only at how we can yank it OUT, without considering why it’s there, what purpose it’s serving. In the terms of buffers, is it temporarily helping someone to tolerate distress? To eat when there’s nothing else? To get rest or escape from their aversive environment? To take up space in their repertoire because there is a lack of meaningful things for them to do, see, say, hear, etc?
Someone wouldn’t use a whole lot of “junk behavior” if their needs were being met, they had tons of skills to communicate effectively, they had meaningful things to do all day and loving listeners to help them spend their time with purpose. (Look at this beautiful way to meet needs WITH “junk” instead of wasting it, and buying yet more building materials!)
The Next Step
Anyway, I hope you enjoy thinking about the buffers today and remembering it’s up to you to do all three: identify your values, understand your context, and design meaningful, committed actions that get you closer to those values. One step closer is enough today. Maybe your step is picking the buffer that most aligns with your core values and operationalizing that one right now! 😊
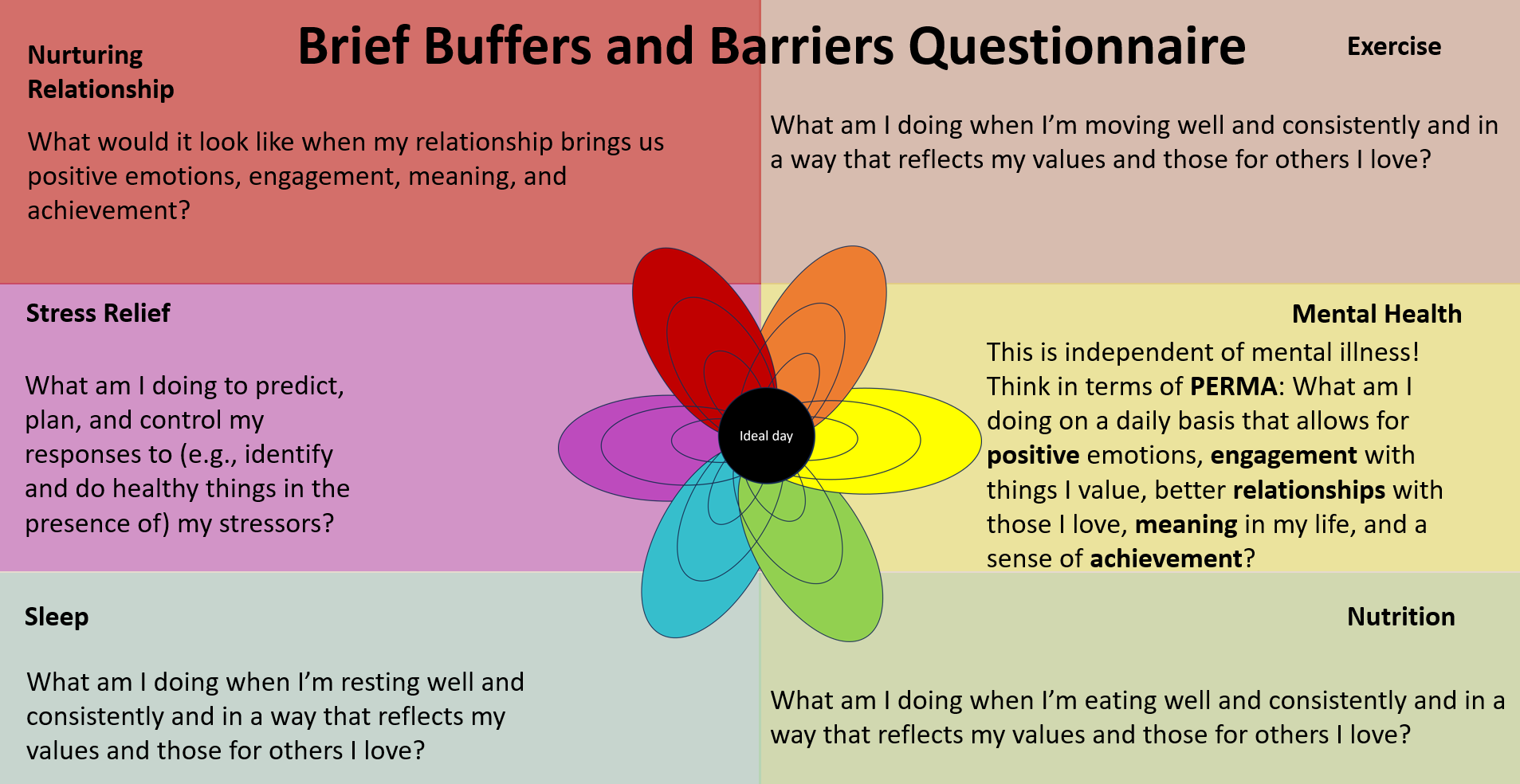
Ready to take Today’s Next Step? Pick ONE buffer below and operationalize it. That means, jot down what it would look like for you to engage in things that reflect your values in this area. What would you wake up and do, and do throughout the day, if your actions in this buffer area really reflected your values?
(An article in the TIBA series by Dr. Teresa Camille Kolu BCBA-D)
One day this spring, Dr. Camille of Cusp Emergence sat down to answer a few questions, and learn a LOT, from Enasha Anglade of LaughLoveLive Again. (You can learn more about Enasha and her work on Episode 87 of the Behaviour Speak Podcast!) Enasha and her fellow researcher and BCBA, Stephanie, talked with Camille about how Enasha’s company and work applies behavior analysis to supporting individuals affected by domestic violence. (And did we mention this dynamic duo will be presenting at BABA this weekend?! Go find them if you’re there!) We also discussed some of the barriers people face in this special context. Not all barriers can be solved with behavior analysis, of course, but there are many things we can do to insure we are minimizing the ones we know about, always staying open to learn about the client’s experience and special context. Each of the headers below reflects an important point heard from Enasha and Stephanie and some thoughts from a trauma-sensitive and behavior analytic perspective.
First, be safe.
Interested in getting involved in working with this population? First things first: it’s really important to be safe for someone. This may seem like a no-brainer. In fact, providing a safe starting place for your therapy is where all trauma-informed support begins, even if (and especially when) your therapy is not treating the trauma itself, but solving problems or building skills or meeting needs related to it. However, there are so many ways behavior analysts violate this number one rule. We might do it unintentionally, such as when we go right to changing behavior instead of listening to a person’s experience and what they truly need first. While there are many trauma-informed resources out there on establishing safety and trust, you can also check out a course on building trauma-sensitive environments (starting with safety), or read a behavior analyst’s discussion on safety in Rajaraman et al.’s 2022 paper on trauma-informed applications of behavior analysis. But don’t skip asking the person how they feel safe and whether there are things you are doing or saying that contribute to their safety or their experience of danger. That’s right- behavior analysts can inadverdently present danger signals to our clients in many ways. When someone is in the middle of a dangerous situation, they are in survival mode and not ready to learn. We don’t want to trigger this for a client and we don’t want to make worse a situation that already exists for them. Being safe (and making sure our presence and therapeutic environment are safe) is not about helping clients avoid all aversive, challenging, or difficult circumstances. Our clients (especially in this context of domestic survivors) are already going through one of the difficult things in their lives. Coming for help and walking out of horrible situations may be even harder than what they’ve been through before… it will be unfamiliar, may be incredibly risky, and may occur at great personal cost to them. What they’re doing is brave. They’re already doing the hard thing. This is about taking their hand and really listening to what they’re going through.
2. Don’t be afraid to go there… but secure support for yourself so your client does not have to do the work for you
Speaking of listening to what they’re going through, behavior analysts can be bad at listening. Does that sound strange? Behavior analysts are great at observing, typically by nature and training… but we can learn to be better listeners, too. And it’s CRUCIAL in this work. Enasha notes that we are often afraid to be personal, to “go there” with our clients. For behavior analysts in the trenches of severe challenging behavior, we’ve often gotten our hands dirty, literally. But to understand our clients coming from domestic violence, being a witness to their story can be meaningful. Listen to your client. Listen long enough to hear. Listen enough to learn what they could benefit from, too. She may need a counselor recommendation, a connection to somewhere she can forge a meaningful relationship, or a tool that you can’t provide (but that someone you know, could). Their daughter may need help for something you don’t treat. Most important, listen to help your client, not just to facilitate your client’s progress with your program.
Related to “going there” with your client, make sure you are not a burden on THEM. If their issues trigger you, your session with them is not the time to discuss that. Of course, there’s nuance involved in learning to listen to someone, so it would be helpful to do any or all of these suggestions: secure your own therapist to go to if you are troubled; be prepared by using specific ACT and mindfulness techniques that keep you able to use your flexibility skills; help your staff debrief with pre-planned supportive interactions after difficult client visits; learn more about motivational interviewing (for a constructional approach from a behavioral perspective see Goldiamond’s constructional interview); and provide training for you and your staff from a trauma expert outside behavior analysis to answer questions about how to support someone disclosing difficult material).
3. Value relationship over rapport, but in the right way.
Of course, if we were talking about real rapport, in the way the layperson uses the term rapport, we’d be talking about the same thing as relationship. The word rapport just means “a close and harmonious relationship in which the people or groups concerned understand each other’s feelings or ideas and communicate well”. But in behavior analysis, the word rapport typically connotes a more transactional process, one used as a procedure as a means to an end. Ultimately, many behavior analysts view rapport as a process one includes in the beginning of sessions or relationships with clients so that clients will be more likely to approach the instructor, and so that the instructor can deliver instructions, reinforcers and other environmental stimuli that encourage the client to change their behavior in specific ways the team has defined and prioritized.
Relationship viewed as an end is different. It has benefits beyond the program. It validates the person and prioritizes their needs. You might think of the way that with a relationship between two people who care about each other, we say goodbye when we’re done. We don’t just transfer off the case without letting the family know because we got a new job, or our hours were cut. However, we’re also not suggesting behavior analysts engage in dual relationships with our clients (an unethical and unhelpful practice to be sure!) What we’re really saying is to value the person over momentary instructional control, and treat them… well, like a person.We still need to be careful, and cautious, to preserve the integrity of precious boundaries. In other words, you are still not going to show up as your client’s “friend”, and you need to teach them, lovingly, how this will work in the beginning of your therapeutic relationship with them. You care about them, and you care enough to support them with their goals. That may include finding friends, or engineering environments that facilitate their making friends, but that’s not you; you’re the therapist. You can still be a good listener, care about your person, and support them without being their friend.
We can program toward the end the entire time, so that there is no disruptive surprise for the client at the ending of the relationship. I like to think about this as fading out interactions to a very low rate that is tolerable, and with programming additional sources of reinforcement for the client. Being the only person your client can trust wouldn’t be helpful; what if you were to have a car accident, move away, or have to reduce your hours? All those things happen, but if you plan from the beginning, you can insure they happen in more therapeutic ways. Be really careful to use ethics code guidelines on transferring cases, especially when you are working with someone in a sensitive and vulnerable situation like those surviving domestic violence.
4. Accept this: any behavior can be influenced both by its consequences in the moment, AND the relevant context and history.
When loud voices in the room ask “what does history have to do with behavior? Shouldn’t we just treat the function that’s controlling it now?”, it can be tempting for vulnerable behavior analysts to question themselves. Should I even be taking a trauma-sensitive approach? Should I take this person’s history into account at all? If it’s just paying off for them in the attention it produces, and we technically know about methods to turn behavior on and off using procedures based on consequences and arranging stimulus control conditions, what does it really matter?
Actually—in terms of bringing up trauma, or changing goals based on it—the answer may vary depending on what the client needs! CuspEmergence doesn’t recommend taking a trauma-informed approach when clients don’t need it. But those going through domestic violence all have been through trauma, by definition. As Rajaraman et al. (2022) states, “Responses to trauma may indeed vary from person to person; however, ACEs are well documented, and a preventative TIC approach would acknowledge their potential impact”.
We recommend behavior analysts working with survivors of trauma be intimately acquainted with the ways trauma relates to behavior, to medical needs, to subsequent challenges and needs, and to the barriers people face in moving on to healing circumstances. (See the sections nearer the end of this article for educating your team if that’s not your forte). And yes, behavior can be influenced by BOTH history (such as the trauma-related factors that were present when someone began to use behaviors that are now difficult for them and they want to change, even if those behaviors are NOW maintained by other environmental factors).
Because behavior is at any moment a function of the dynamic interaction between the local and historical context, it is possible that the intervention strategies identified during the functional assessment phase as “likely to be effective’ will need some modification when it is actually time to intervene. As Stephanie notes, clients affected by domestic violence may face unpredictable and changing needs. The needs of the client demand that the analyst be flexible and sensitive to the contingencies and challenges our client faces. We should be especially focused on tracking the ways we might be contributing (perhaps unintentionally) to coercive cycles of interaction for our client, perhaps hindering their growth by playing in to a power differential or offering choices using an architecture that WE don’t perceive as, but the CLIENT experiences, as coercive.
5. Identify the basic training your team will need. What are the most essential and meaningful training components your staff will need? Who provides that training, and how can you value it at the levels of culture, group, and individual?
What happens when most of the team cannot relate to the particular difficulties with which a client is struggling? They might recommend changes that are not feasible to the client; they might miss danger signals the client is sending based on what is happening around the client (and miss an opportunity to prevent harm); they might take personally or misunderstand the challenges a client is having and miss crucial chances to intervene appropriately; they might cause harm by actions intended to help; and so much more.
One team we know used to have a person on staff who provided this training because she had been through it, but her caseload is now too big for her to spend time with each new staff person. As the team grew, the personalized approach they were known for was eroded and eventually, the services they provided looked like most other agencies, and they were no longer meeting the individual needs of client families. However, they didn’t know it until they received feedback, because nothing had been intentionally changed; it was simply a product of drift that happened with the welcomed growth going on.
So one solution for teams with similar paths is to prioritize providing training from a reputable and experienced source, and doing that both routinely and in a way that continues to answer questions the new team members will have as they gain their own experiences and put their previous knowledge into their new context. In a subfield like domestic violence, this training needs to come from someone either outside of behavior analysis, or from someone whose training, expertise, experience and culture strongly intersects with that of the clients and their needs. If this person is not on staff, it is essential to secure regular training, as well as embedding this as a priority into the agency’s mission, core processes, values at work, and interacting with clients. Staff should not have to ask for designated and regular times they will be paid to access and discuss and apply the training (and receive appropriate feedback from someone equally experienced and trained).
6. Identify the most important kinds of support your clients will need that you cannot or do not provide. What kind of support is needed, who else provides it, and what would you like to be doing in 5 years if you removed barriers related to this support?
The first part (who else provides this?) is a logistics question. Prioritize finding those answers right NOW. If most of your clients receive behavioral support from you, but also need to be able to access certain other resources to survive, find out all about those resources and who provides them.
The idea is that you can position your agency in the middle of a network to which you can connect your clients. You do not want them struggling, alone, with something that could make or break their ability to come back to access your services or to implement them. We can start small, beginning with very simple connections you provide your client, such as a list of websites, phone numbers and connection names for partner agencies in your area that meet big needs (and funding options for those needs).
The second part (what would you be doing in 5 years if you removed obstacles?) takes more planning, but might make sense strategically depending on your clientele and their challenges. Some of the solutions could include creating a part- or full-time position of Resource Coordinator, hiring a social worker, or forging a strategic partnership with someone who fills this role for other companies and who knows your area well and can devote time to your own clients on a weekly or regular basis that makes sense for your client volume.
Do you do this work yourself? Contact us and add your essential strategies. Want to learn more? Find Enasha and Stephanie at BABA, listen to the podcast (Ben is in Detroit right now documenting BABA 2023!), follow ACES and ABA groups on social media, send us a comment and leave us your email below, or take a course on trauma sensitivity. We hope to hear from you soon!
Specific buffers (see Purewal et al., 2016) can actually protect against the harmful impacts of ACES on medical health. The particular buffers found to reduce harm include getting enough sleep, eating nutritious food, having access to mental health care, experiencing a safe relationship with someone, exercising regularly, and practicing stress relief techniques that allow someone to experience calming down (such as a simple mindfulness technique). Adding buffers may be a set of seemingly small actions, but they contribute to preventing problems from becoming larger, and may help solve challenges related to why a behavior plan is just not working. (Solving basic problems in the behavioral environment regarding access to needs can be an area consistent with the ethical imperative behavior analysts have to address conditions interfering with service delivery; see BACB, 2020, 2.19).
Although the buffers make a big difference in preventing from harms and protecting against future ones related to ACES, many individuals and families face major barriers related to access, information, resources, or behavioral needs. These barriers can reflect resource inequalities, individual differences, and cultural challenges that prevent many from experiencing the benefits. How could we leverage “buffers and barriers” policies to protect against harms (and truly embody the preventative arm of behavior analysis)?
One of the difficulties with beginning to implement buffers for individual clients is that behavior analysts may be hesitant to devote precious resources to this new and potential preventive area. To assist teams in understanding further how policies might affect our clients, their caregivers, and our staff, Cusp Emergence is engaged in developing resources and collecting feedback about their use. Some of the resources provide examples for conversations we could have with others, while others are visuals to help others easily understand the buffers and barriers (such as the “Be a buffer. Solve a barrier” downloadable pdfs in this article). We also have lists of policy ideas for interested agencies, risk benefit assessments to aid in their implementation, and examples of how we define buffers for individual clients, families and staff. Use our contact us form below to let us know which resources are your favorites or what else would help you more actively approach this area. Oh, and stay tuned for more on this incredible topic. Soon we’ll be be exploring buffers in more detail, including sharing some ways we integrate it for our clients, how it can be meaningful for caregivers and staff, and some of the research on each one.
For me, an on-demand workshop does several things: It can be taken any time; one can take it with a group and apply exercises with other people if desired; but since it’s on-demand, an individual will benefit even if taking it solo. It should be expandable if one wants to be able to sit with a chapter for a few extra hours because we simply love the content; there will be resources to grow with and come back to if one can’t do all the exercises right NOW. I’ve been on sabbatical a while; as I return to doing interviews, conferences, talks, and podcasts (including a new one we taped recently for the Atypical Behavior Analyst, with my friend Dr. Eddie Fernandez airing later), it is nice to be able to take something on my own time, when tiny folks are asleep, and I know many parents – and folks going through school and work at the same time – are in the same boat.
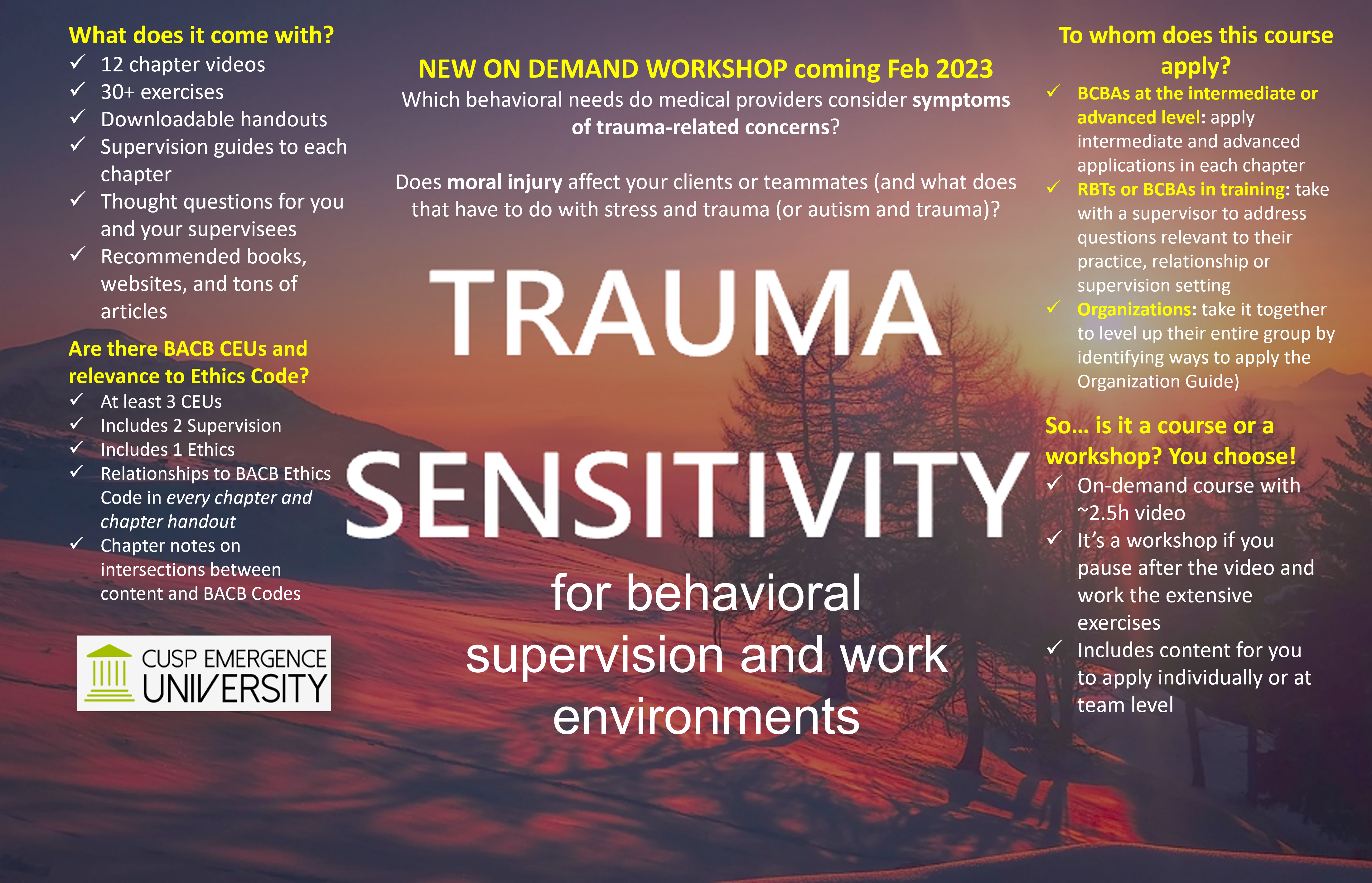
30+ exercises with the videos: Because this is an on-demand workshop, we present a TON of exercises packaged with the videos. Teams or individuals can easily do a chapter a week along with exercises for a truly transformative experience in your office or supervision setting. But if they choose to take it all at once in an afternoon, that’s possible too. So it’s customizable.
Scalable applications for team members, supervisors and supervisees: The new content (on leveling up the trauma sensitivity of our staff and client environments) is “scalable”, meaning we include applications for 3 different levels of staff: those in roles that are basic; intermediate; and advanced. Presenting it as a workshop meant that the team members “leading” the discussions and exercises benefit just as much as (but different from) the less advanced team members they are mentoring through it.
Supervision guides and chapter handouts: These come with every chapter video and walk the student through the material, from the main ideas we presented, to definitions for any new vocabulary, exercises, lists of Ethics Code items that relate, thoughtful discussion questions, exercises, and chapter resources and articles. Every chapter comes with its own handout and supervision guide to help BACB supervisors or team leaders support our coworkers and supervisees.
The two things I personally love most about this workshop are:
it addresses tough topics like moral injury with your team members and considering how this ethics area could apply to our supervisees but our clients too;
and we provide resources to follow up on big ideas like this one: there are some behavioral needs that medical providers consider symptoms of trauma-related concerns. (If folks are new to integrating trauma sensitivity in their supervision and client environments, we might miss this huge opportunity to make sure we do no harm by treating behavior needs that are actually related to new abuse.)
Wondering about the content of the new workshop? Here are the chapters (each has its own video, ethics intersections, resources, thought questions, and exercises):
Chapter 1: Principles of Trauma-Sensitive Care
Chapter 2: Interactions that could help or do harm
Chapter 3: Features of trauma-related responding
Chapter 4: Defining trauma
Chapter 5: Risks related to trauma
Chapter 6: Elements of a potentially trauma-related response
Chapter 10: Want to mitigate risk? Document it first
Chapter 11: Skills and Stress
Chapter 12: Healthy Collaboration
Above: Table of chapters from Trauma Sensitivity in the Behavioral Workplace, new on-demand workshop from Cusp Emergence
Did you enjoy this article? Come back soon when we’ll cover a few more related topics including: mentorship groups for those applying trauma sensitivity principles in their supervision sessions; how to get the most out of your workshop experience by doing exercises as a group or dyad; more info on a brand new all-trauma conference coming in April hosted by the formidable Dr. Gabi Morgan; meetups in Denver May 2023; and more!
Read below for final thoughts and some links if you’re in the market for values related CEUs: Recently, when my own CEU cycle was about to turn over, I knew it was time to take a course or workshop in something I could use NOW and am passionate about… so I went searching for three things: supervision CEUs; offerings from people I admire and from folks who literally wrote the books on leveling up mentorship and supervision and working with families; and opportunities to learn about values in a deeper way that would help me level up my own practice. That led me to a couple of great courses and podcasts; one of these opportunities was a workshop with built in exercises that could be taken quickly or over the course of a few weeks and included opportunities to network with other folks. It was a really lovely experience. Included are links to a couple trainings and podcasts from respected folks who continue to inspire, below.
Last time I wrote, I shared some ideas about this intersection. Today, the new course is up! Before you go check it out (and claim your February 2022 coupon for 20% off by typing ASD2022)– during the introductory month of the course)- learn why I’m so passionate about screening for trauma in a population so many behavior analysts have been working with (for some, virtually their entire professional lives).
Have you ever worked with someone in pain? How do we know if they’re currently hurting, whether it’s because they are sick, it’s related to interventions we chose, or from experiences we reminded them of? How would we know if that was the case? Did that person cower, freeze, or grimace? Did they flinch, close their eyes, seem to “zone out”? Perhaps someone has run away, played repetitively with the toys they had, or fallen asleep at school? Sometimes, respondent behaviors may be giveaways that people are experiencing fear or in pain, but successful avoidance behavior can hide that pain. Other times people have been through experiences making them more likely to use aggression or property destruction. In the least, we should consider whether our interventions cause harm. This harm could include causing our clients distress or pain, exposing someone to additional risks, detracting from their quality of life, failing to program in sustainable ways that transfer to the maintaining environment, and so much more.
A new training is up on Cusp.University on the intersection of autism, trauma informed behavior analysis, and ethics. By the time we near the end, we have discussed and revisited the idea of contra-indicated procedures. Given that lists exist for diagnoses of autism alone, why isn’t there a list of best practices appropriate for clientele meeting diagnostic criteria for autism who also come to therapy with trauma histories? Why is it so difficult to find articles suggesting best treatment paths for individuals with both autism and trauma related experiences in the literature? In behavior analysis, answers to these questions may be related to our field, its historical publishing practices, and the ethical and pragmatic need to individualize procedures for each client.
In terms of publishing practices, a panelist in ABAI’s “Exploring Publication Bias in Behavior Analytic Research” (which included Galizio, Travers, and Ringdahl, 2021) stated,
“No intervention is guaranteed to work for every individual, every time, in every context.”
They suggested that authors writing about their research should include more detailed descriptions of the conditions under which successful implementation of the intervention occurred.
When we screen for trauma related or aversive historical situations and stimuli, we often learn things that
help us prioritize treatment,
document risks for certain procedures,
avoid or prioritize certain stimuli,
detect environmental conditions that are acting as motivational operations and conditioned MOs,
and ultimately, perhaps minimize harm to our client.
Screening for trauma can help to identify individuals with prior risk factors who are at risk for experiencing additional adverse events and aversive conditioning. Attendees learn in chapter 1 some facts about how being autistic is to be at increased risk for trauma, bullying, abuse, increased likelihood of experiencing foster care—and in chapter 3, learn about the higher rates of experiencing restraint, seclusion and being excluded from school.
But another effect of screening – one that should affect all behavior analysts—could be an increased awareness of the fact that behavior analytic procedures are being used all the time for this population at the intersection of autism and trauma. Perhaps the least we can do is to begin doing behavior analysis with people instead of to people, and to be transparent, inviting, and open in looking at options—and their likelihood of causing harm either now in the future.
Let’s look at this juxtaposition: we have a great ethical responsibility to do no harm, but also an ability to cause great harm. With using any behavioral procedure there comes a risk that we may do just that. This is especially true when we don’t have literature evidence that a given intervention is appropriate and effective for the person’s needs given their history and current situation. Perhaps they don’t actually need behavior analysis seeking to change their behavior as much as they need a roof, a meal, a bus pass, a blender, a respite provider, a ride to the doctor, a coat, a medication, a trip to the dentist… the list could go on and on. So clearly the first step is to see what the person needs.
When designing an individualized behavior support plan, two things are important to consider:
(1) the risks and benefits for the client themselves, given their needs, values, environment, etc., (e.g., the long- and short-term outcomes of procedures and decisions, and
(2) evidence the procedure is appropriate for our client.
In terms of evidence, when considering decisions in context of the literature, few studies provide sufficient detail in characteristics of the participants. So it is difficult to tell, reminds the panel, which characteristics were present for study participants received successful or unsuccessful interventions. Thus we can’t really tell how many of the massive number of papers on treating behaviors in autism, also apply and were conducted with individuals with autism who also had a trauma background. But statistics suggest many of them must have. In the science of behavior analysis, each subject’s behavior is its own control, so if we control our conditions and try to measure well, we may reveal additional elements of historical and current behavioral environments that exert contextual and stimulus control on the client’s behavior- and that change their needs. At times, historical aversive conditioning experiences may have contributed changes making it painful or inappropriate for clients to experience certain interventions. As we discuss in the new training, some of those conditioning experiences may even have occurred during and as part of behavioral treatment.
We can’t know for sure what our clients have been through. But when owe it to them to honor those experiences if they are comfortable sharing them.
Here are some of the things you’ll learn.
Course Objectives:
1. List connections between autism and trauma in the research
2. State different kinds or examples of trauma that may affect individuals with autism
3. State supportive ways to ask about trauma histories
4. Select examples of how medical history can be related to trauma
5. State examples of repertoires beneficial for practitioners who serve clients affected by both autism and trauma
Ready to learn more? The new training offers hints from Dr. Kolu on how we begin the conversation about informed consent and screening for trauma, why assent is so important, how trauma and autism might intersect with medical needs affecting our clients, and more. And all the resources are available as free content in the preview section, so go grab that now! See you at a conference soon or find us online. And thank you for listening!
These findings are some of the reasons researchers (as well as research-practitioners, including those of us at Cusp Emergence) urge practitioners to adopt screening in order to support the huge group of people affected by both trauma and ASD (see Brenner, Pan and Mazefsky et al. on the need for screening, and special behavioral differences that occur in this population).
ASD and TIBA: Our newest upcoming course on CuspEmergenceUniversity.com
They are also just a few of the things you’ll learn when you take the upcoming course on CuspEmergenceUniversity on trauma and autism (coming Fall 2021). Other topics we cover include:
-client examples from both child and adult populations whose experiences include autism and trauma
-literature references helping practitioners discover more about what trauma related experiences people with autism may face
-how behaviors themselves can be risk factors for additional trauma
-behavior programming examples that may be counterindicated procedures depending on the individual needs of autistic people who faced trauma
-examples of ASD communication needs that have been particularly helpful to target when supporting this population after trauma
-behavioral cusps that can make a huge difference after trauma
-examples of worst case scenarios people face when trauma history is not taken into account for individuals with autism after trauma….
…and much more. We also cover how Cusp Emergence uses the SAFE-T model and Assessment (including our risk versus benefit tools) to be more supportive, mitigate risks unique to autism and trauma, and learn more about the whole person and their needs.
This is the 21st article in a series on Trauma-Informed Behavior Analysis by Dr. Camille Kolu, BCBA-D
I often hear from educators and behavior analysts, “What do you actually do differently if your client has faced trauma, given your role as a behavior analyst?” In this bulleted series we’ll get there, but we’ll start with what I would want you to understand about myself as your client (or teammate!) who has experienced adverse experiences. Here we list 25 different things I want you to know. (As a hint, each thing we can understand about a person could be a bridge, if you choose to walk through this difficult thing to a shared place of understanding on the other side. We’ll explain in more detail in future posts, or you can check out our course library over at CuspEmergenceUniversity if you’re interested in expanding your boundary of competence). But first,if I were your client or team member – if my past involved trauma – I would want you to understand thatnow, with the presence of historical trauma,
I MAY:
have difficulties calming down when under pressure
have difficulties using “appropriate” behaviors even after years of programmed reinforcement for using them
have mental health concerns that have never been appropriately addressed because my behavior masks my needs
find some kinds of social interactions difficult or painful
have trouble controlling some of my bodily functions, but may not be able to describe to you why
experience “triggers” in the environment that you can’t see (but that an experienced provider could locate, document, and learn to help me explore or move with, as appropriate)
experience some times of the day, week, month, or year that are marked by aversive events for me that you won’t know about
may not be able to explain WHY this time is difficult or why I am using an “old pattern of behavior”
find it more difficult to perform, or to learn and remember new things than others of my age, skill level, or occupation – even if “on a good day” I can do this just fine. (By the way, have you read The Four Agreements? Do you know how important it is to take nothing personally and know that others are doing their best (and how critical it is for you to do the same)? If not go check it out.
use occasional behavior that is mistaken as “ADHD” or “ODD”, or more, but that is actually related to how I was mistreated
have been given misdiagnoses, treatments that didn’t work, or medications that made my problems worse or that interacted with each other in harmful ways that hurt my body and cognitive function
attempt to advocate but get ignored when I try to communicate pain, mistreatment, or a medical concern
be more likely to experience FUTURE trauma because of what I faced before
lack a reinforcing and useful repertoire (e.g., full complement of skills and things to enjoy), especially if I faced treatments that just tried to “teach me a replacement behavior” for a few challenging things I did, instead of understand and grow me as a person in the context of my own community, needs and desires for my future
be part of a long line of marginalized people or one of multiple generations exposed to trauma
have a chance to change our lineage… if you help
After all, I AM:
a human being with interests, feelings, and great potential for growth and joy
more likely to experience certain risks (I may be at greater risk of losing my educational or therapeutic setting, go through harmful discipline practices, be exposed to law enforcement interaction, for example)
in need of understanding, an informed supervisor and system of support, and someone who will document my challenges so we can work on them, but not emphasize them so much they ignore my strengths, needs and skills
capable of much more on my best day than I show on a hard day… but I am always doing “my best” at the time, given what I have been through and what I AM going through, and despite what it looks like
Taking these points as a starting place, future posts in this series explore what I NEED as a person who may have faced these things, and what I DO as a behavior analyst who cares. We’ll also share some of what I need from my supervisors or systems administrators! What would you add to this list? What are some of your action items?
It’s finally here! We have learned so much from workshop attendees, trainees and supervisees in this area over the past several years, and appreciate the attendance, feedback and support of everyone who has taken the training or used a version of the SAFE-T Assessment. Coming on Monday, the booklet and training for assessing trauma-related factors affecting our clients of behavioral services, are available ONLINE as a self-paced course. This course provides a download of the new and expanded SAFE-T Checklist booklet, which contains several tools enabling the screening and documentation of over 200 trauma-related factors, and a Risks and Needs form to help teams understand (and document) how these factors confer risks (and converge in risk factors that must be solved or mitigated to protect our clients, teams, and ourselves). The booklet contains an extensive reference section and team supportive tools as you use your new knowledge to better align your team’s skillset with the Ethics Code, and the individualized needs of behavior services clients after trauma.
Severalof our behavior analytic and collaborator clients across institutions, educational facilities and private companies clients have shared that learning to assess risk factors related to trauma, and to apply this information to their teams’ FBAs and risk mitigation plans, took their skillset to the next level – essentially affording them an opportunity to acquire an important behavioral cusp for their teams.
Some new components of the booklet include:
An optional buffer/ resilience score to assess whether protective environmental and therapeutic components of a client’s plan are in place (to understand some ways that trauma gives rise to medical and behavioral challenges and some buffering factors that can help, please see the book or scholarly articles by Dr. Nadine Burke Harris (e.g., Oh D.L. et al. 2018), who is the Presidential Scholar for 2021’s upcoming Association for Behavior Analysis International’s conference. She will address the critical topic of breaking the intergenerational cycle of adversity, and screening for ACES (adverse childhood experiences).
Information about over 50 risk clusters (groups of related risks in the 6 assessed sections of the SAFE-T Assessment)
Cross-reference tables showing, for each item we screen for, the location(s) in the SAFE-T Checklist
Infographic on components of a trauma-informed FBA
Brief templates for Risk Versus Benefit Analysis and Risk Mitigation Planning
The IPASS (Inventory of Potential Aversive Stimuli and Setting Events) tool and instructions
References (organized by topics) covering over 40 areas or topics of literature related to trauma (including relationships of ACES to medical problems, ACT and intellectual disability, ACT and anxiety, foster care and adoption, the relationship of abuse to pain, drug use and trauma, and much more).
Time required: The course includes about 4.5 hours of video content in 12 lessons, each followed by a brief quiz.
This is the 20th article in a series on Trauma-Informed Behavior Analysis by Dr. Camille Kolu, BCBA-D
In medicine, contraindicated procedures are those that are withheld due to the potential harm they might cause to a patient. More and more, behavior analysts are interested in learning about someone’s history, in part to lessen the risk they will do a client harm.
We are tasked, ethically, to do no harm (and see the BACB Ethical and Professional Code item 4.02); to evaluate potential risks and side effects of interventions and to weigh the possible benefits of each (see 2.09 and 4.05); and to avoid using harmful reinforcers or those that require excessive motivating operations to be effective (4.10). For RBTs as well as those certified at higher levels, ethics obligates us to protect our clients from harm (see RBT Ethics Code section 2.02).
In our live webinars (please see CuspEmergenceUniversity.com where we list topics we train frequently on– any course you see there is available as a live webinar training or, in some cases, available as an on-demand training), we receive frequent questions like this:
What kind of procedures should be avoided when working with a new client after certain types of trauma? Are there certain procedures we should give more thought to after a client has been through challenges we know about? What do we do if so?
Given these wonderful questions, today’s post shares a few basic procedures that may be contraindicated – at least at first—given a specific combination of historical factors involving trauma.
Of course, it’s not black and white. Often this should just be the first step for the team, a conversation in which people consider potential for risk conferred by historical variables. The team can then make a more careful decision in order to mitigate possible risks and maximize the benefit of any procedures selected, along the lines of what our code suggests in item 4.05. Though each procedure below is potentially contraindicated at first, it could be appropriate later in treatment, or perhaps from the beginning- the point is that this should depend on an individualized risk versus benefit analysis of the other options available to the team, the client’s history and needs, the severity of the past abuse or neglect or trauma, etc.
For a client who has experienced previous food insecurity, food related abuse or neglect, and/or severe food deprivation:
One potentially contraindicated procedure is using edible reinforcers.
Notes: Here there are risks to the client, and also potential risks to the client’s relationship with their caregivers and team members. The conditions necessary to establish the motivating operation for reinforcement may be similar to previously neglectful or abusive conditions, or may act as conditioned motivating operations that make harmful behaviors temporarily more likely. In our history treating clients after these circumstances, we have also experienced something related to behavioral contrast in this situation. For example, a client who was provided edible reinforcement in their new applied behavior analysis setting then went home and used dangerous and surprising behaviors related to their neglectful history. The client’s foster family was caught off-guard by these new behaviors, but they could have been predicted during team education on how edible reinforcers might need to be avoided at first when conditioning new team members as reinforcing (and as instruction-related discriminative stimuli).
2. For a client who has been involved in previous sexual abuse (including when the client also makes allegations):
One contraindicated procedure is assigning a 1:1 without additional oversight.
Notes: Here there are risks to both the client and additional team members. When the team receives this case, it would be contraindicated to immediately assign 1:1 support without preventative measures such as training for the 1:1 and supplemental recording, additional oversight or whatever is deemed necessary.
3. For a client who has experienced medical complications from sexual or physical trauma (e.g., this could include incontinence, fecal smearing or related concerns, etc):
One contraindicated procedure is conducting toilet training without oversight from a medical professional, additional training or consultation by someone with expertise in this circumstance, etc.
Notes: In this situation, respondent and operant interactions can occur that are dangerous to treat without expertise; the client can risk serious complications and worsening medical problems; there is a risk of further conditioning the experiences of voiding (and related rituals) as aversive; there is a risk of occasioning behaviors related to the past abuse, or pairing aversive events with team members involved in the procedures; and more.
4. For a client who has experienced previous neglect or adverse circumstances (such as deaths of parents, removal from unsafe conditions, or experiencing war, dangerous immigration or poverty related issues), resulting in deprivation of basic needs and social interaction:
Some potentially contraindicated procedures involve attention related extinction, differential reinforcement of appropriate versus inappropriate requests, or time out from attention reinforcement.
Notes: In this situation, there are safer procedures to begin using that could avoid some of the harmful side effects of removing attention contingent on unsafe behavior. A child with a serious history of neglect may have used behaviors that can seem bizarre or out of context for typical child development, but that were critical to the child’s survival. At the same time, it may not be appropriate to pair new team members with procedures that were used in the child’s neglect, even if the “intent” is different. There are many procedures that can be used more safely, such as using enriched environments and fixed time schedules, to provide monitoring, insure high levels of safe attention, and begin to condition adults as neutral stimuli again, if needed, after harmful interactions with adults in the person’s past.
5. For a client who has been affected by physical and/or sexual abuse, behaviors and circumstances consistent with reactive attachment disorder, or multiple and changing caregivers in childhood:
One potentially contraindicated procedure might be contingent praise statements to establish compliance related behaviors.
Notes: In this situation, a client may have had a history in which adults could not be trusted, behaved inconsistently or inappropriately, or paired unsafe and harmful actions with typical caregiving behaviors. Clients who experienced this may initially present as lacking “a compliance repertoire”, but it may be contraindicated to attempt to establish and praise compliance, for several reasons. Some may be overly compliant, and lack self-help and self-advocacy repertoires that are critical to autonomy; if they are still going home at night after the school day to an unstable situation or multiple foster homes, to praise rigid compliance may increase the risk of further victimization or contribute to future abuse. At the same time, initial praise for compliance may damage relationships between the client and new caregivers who have not “earned” the right to praise the client’s behavior by establishing a history of consistency and helpful interactions. Furthermore, praise might already be conditioned as aversive for the client and could sabotage the caregiver’s attempts to establish a relationship or instruct appropriate behavior. (CuspEmergence.com has written elsewhere about praise here).
6. For a client who has been affected by neglect, and involved with law enforcement, suspensions and challenging behavior:
A potentially contraindicated procedure is least to most punishment.
Notes: Implementing punitive procedures (or procedures that educators assume to be aversive and are using to control behavior) in a “least-to-most” order is dangerous, especially after the interactions mentioned here. Any time punishment is implemented in a LTM order, we risk these outcomes: conditioning the aversive stimuli becoming more reinforcing, and more familiar; worsening the client’s behavior as they need to contact more and more of the supposedly aversive stimulus; pairing the people administering the punishment with aversive control, making it more likely the client will (to speak loosely) act out more and more for their high-quality attention; etc. (CuspEmergence.com has written about the potential pipeline from special education to prison here, in an article referencing some of these concerns and containing behavior analytic references.)
7. For a client with symptoms or diagnosis of trauma-related disorders or needs:
A potentially contraindicated thing to do is recommending or implementing applied behavior analysis without any mental health or trauma-focused treatment or input.
Notes: Behavior analysis (at least the kind I provide and teach about) is not a trauma treatment. We are also not a source of diagnosis for trauma. Instead, I work in a complementary way with a team and/or family that is interested in learning about risks related to trauma history, and how these risks affect the person’s behavior, needs, and supports. There are therapies that can provide trauma-focused treatment and aid a person to heal after experiencing difficult circumstances; a person may need these in addition to, or before, receiving behavior analysis to aid them in developing a safe, expanded behavioral repertoire. If someone trusts you with their trauma history, please be careful and supportive.
In closing, for a client with a specific conditioning history, the contraindicated procedure would likely involve aversive conditions and potentially medical or biological variables. Always consider items 3.02 and 4.08 from our Professional and Ethical Code, and discuss whether they apply to your case:
3.02 Medical Consultation. Behavior analysts recommend seeking a medical consultation if there is any reasonable possibility that a referred behavior is influenced by medical or biological variables.
4.08 (d): Behavior analysts ensure that aversive procedures are accompanied by an increased level of training, supervision, and oversight. Behavior analysts must evaluate the effectiveness of aversive procedures in a timely manner and modify the behavior-change program if it is ineffective. Behavior analysts always include a plan to discontinue the use of aversive procedures when no longer needed.”
Behavior Analysis, Aging, Trauma, and Supervision (or BATS, in honor of Dr. Janet Ellis).
This is the 18th article in a series on Trauma-Informed Behavior Analysis by Dr. Camille Kolu, BCBA-D. It includes something new that we have been asked about: Companion notes for students and supervisees working through this information with the support of their supervisor.
I heard Jon Baker give a great talk on advances in behavioral treatment of gerontology the other day at COABA. It made me think of my students at the University of Colorado Denver and our supervisees. (There was also a fantastic talk on supervision and feedback by the incomparable Ellie Kazemi, whose book on supervision is out now). When they ask about clients other than autism who have benefited from applied behavior analysis, my supervisees are usually excited to read stories in which ABA changed the lives of people with dementia, brain injury, medical needs, and more. For example, an article from Baker (2006)Continue reading →














{kind=link}
{kind=link}
{kind=link}